When I was trying to tidy up the previous blog post “How to protect yourself and the people you love from lead poisoning”, a few things came together. If you’re not interested in workplace health and safety, please scroll down to the bottom of this blog post and you’ll find out how to protect yourself from lead.
My journey of learning about lead and chelation started back in 1982 with a break between then and now. In the interim I’ve learned quite a bit about lead toxicity, and the exposure to lead that all of us face, with lead risk workers on the front lines, and also how lead exposure might be something we can face without any harm.
Of all the things that bother me about the failure to properly address exposure to lead, it’s that despite knowing the harm that lead can do, next to nothing is done to alleviate the effects of lead, particularly in children. This doesn’t need rocket science, or new drugs and treatments, all it needs is applying what we’ve already got and learned in the last 60 years. Why is that too hard?
I started this blog to hopefully force, embarrass or whatever a change to the existing workplace health and safety regulations about lead risk safety monitoring. I have a relative working in Mt Isa and a conversation with him caused me to check what the regulations were. They were insane in my opinion because rather than “protecting” lead risk workers, they were doing the opposite, because they ignored the fact that the fall in blood lead levels (BLL) when a worker was removed from lead exposure wasn’t due to lead leaving the body, which it doesn’t for the most part, but was due to lead moving elsewhere in the body, like soft tissues including the brain, and finally to bone. Lead mimics calcium in the body, and like calcium, it’s retained in the body.
An absolutely beautiful example of how little progress there has been in the workplace health and safety (WHS) are when it comes to lead risk workers is this 1980 US OHSA incident report which uses regulations that are still in place today:
Lead is eliminated from the body via urine and feces. NIOSH recommends that a blood lead value of 60 micrograms per 100 grams whole blood (60 ug Pb/100 g blood) be the maximum occupational blood lead level. When this value is exceeded, the employee should be removed from the lead exposure to allow his body to reduce its lead burden.
Here we are 43 years later, and the BLL level for lead risk worker removal is still only half of what it was in 1980 and is still based on the absolutely inexcusably stupid assumption that lead rapidly leaves the body when we’ve had 43 years to correct that error. Would any organization that cared about worker safety ignore a basic problem for 43 years?
Removing a worker with a BLL over 30ug/dl from exposure doesn’t do a damn thing to reduce the body burden of lead. Removal is not a protective action. If anything, it’s a penalty applied to the employer which may in fact not be inappropriate. There are minor losses of lead when red blood cells containing lead are broken down, but the bulk of the lead is there for decades, maybe your whole life.
Your’e probably sick of seeing this diagram, but it’s a great way to illustrate where you are with a BLL over 30ug/dl, pretty much screwed.
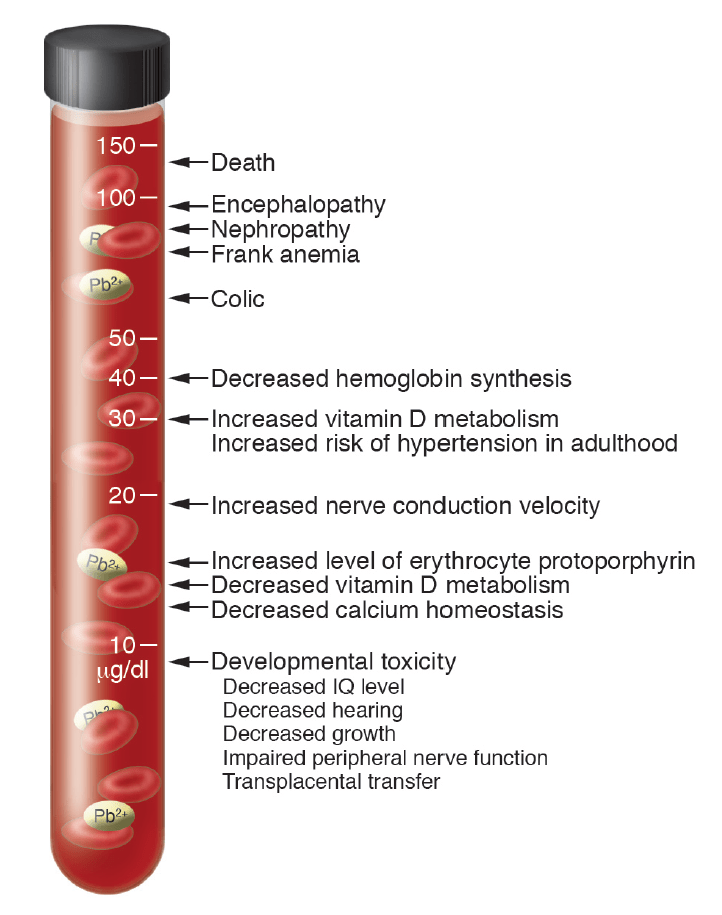
At about 15ug/dl, you’re seeing all the sub-clinical symptoms that indicate excessive lead exposure. At 30ug/dl, you see increased blood pressure, increased rates of cancer, a doubling or trebling of the risk of dying of cardiovascular disease. Simple stuff.
The problem was so obvious to me that I stupidly assumed that if I explained what was wrong in a simple enough way, people would realise that they were harming workers and do something to fix the problem. After all, that’s the role of people in WHS isn’t it? They’re supposed to protect workers and promote a safe work environment?
Wrong. Think about the role of HR (human resources). They’re not there for the benefit of the workers, they’re there to manage the workers on the bosses behalf. WHS is there to do the minimum amount they can within the regulatory framework defined by government agencies. The easy stuff gets done, the more complicated stuff like biohazard monitoring, has to appear as if something is being done, even if it results in harm to workers.
I’ve yet to encounter an organization; Glencore, Resouces Safety and Queensland Health, or Safe Work Australia, that did anything but pass the buck. Mt Isa Mines or Xstrata, before Glencore took over, might have done something but we now have Glencore. Glencore don’t seem to want to know, especially since there’s another little issue arising in Townsville where Mt Isa has been shipping lead ingots and concentrates for the last 90 years.
In the case of Safe Work Australia, they’re quite happy to admit that there are problems with lead biohazard management in their documentation, but that concern isn’t reflected in their model regulations which are the basis of regulations used by all the states (and NT) except Victoria. The existing lead risk worker “safety” regulations use lead risk workers as “mine canaries”.
Lead risk worker safety, or more correctly protection from harm, is obviously too difficult to even consider. RSHQ (mining WHS, Queensland) has a logo that says “ZERO SERIOUS HARM”. Considering the serious harm lead can cause in lead risk worker’s bodies, and not even considering if one of them is a female of child-bearing age, this logo is a blatant lie if it represents RSHQ stated aims, and a bad joke regardless.
I’ve said all this before in other posts, but why bring it up again now?
Well, it’s because things could be even worse.
I started looking at some of the international WHS sources, and I came across a section of the US Occupational Health and Safety Agency standard about lead “safety” that nearly blew my mind. As you’d know I’ve been proposing chelation to remove lead as a solution to avoid the ill effects of lead. The OHSA documentation t basically absolutely disallows using chelation therapy for anything but severe lead poisoning.
I’d like to quote some of it below (the bolding is mine):
The medical surveillance section of the standard also contains provisions dealing with chelation. Chelation is the use of certain drugs (administered in pill form or injected into the body) to reduce the amount of lead absorbed in body tissues. Experience accumulated by the medical and scientific communities has largely confirmed the effectiveness of this type of therapy for the treatment of very severe lead poisoning. On the other hand, it has also been established that there can be a long list of extremely harmful side effects associated with the use of chelating agents. The medical community has balanced the advantages and disadvantages resulting from the use of chelating agents in various circumstances and has established when the use of these agents is acceptable. The standard includes these accepted limitations due to a history of abuse of chelation therapy by some lead companies. The most widely used chelating agents are calcium disodium EDTA, (Ca Na2 EDTA), Calcium Disodium Versenate (Versenate), and d-penicillamine (pencillamine or Cupramine).
The standard prohibits “prophylactic chelation” of any employee by any person the employer retains, supervises or controls. Prophylactic chelation is the routine use of chelating or similarly acting drugs to prevent elevated blood levels in workers who are occupationally exposed to lead, or the use of these drugs to routinely lower blood lead levels to predesignated concentrations believed to be “safe”. It should be emphasized that where an employer takes a worker who has no symptoms of lead poisoning and has chelation carried out by a physician (either inside or outside of a hospital) solely to reduce the worker’s blood lead level, that will generally be considered prophylactic chelation. The use of a hospital and a physician does not mean that prophylactic chelation is not being performed. Routine chelation to prevent increased or reduce current blood lead levels is unacceptable whatever the setting.
The standard allows the use of “therapeutic” or “diagnostic” chelation if administered under the supervision of a licensed physician in a clinical setting with thorough and appropriate medical monitoring. Therapeutic chelation responds to severe lead poisoning where there are marked symptoms. Diagnostic chelation involved giving a patient a dose of the drug then collecting all urine excreted for some period of time as an aid to the diagnosis of lead poisoning.
Why would any authority consider that chelation treatment to remove lead is only justified at the point where gross injury is likely and for no other reason?
There were a number of clues, but the comment about the history of abuse of chelation therapy was the key. What was that about?
It seems that some lead companies tried using chelation therapy as an excuse for not having to reduce lead exposure in the work environment, and some other companies genuinely tried to reduce the amount of lead in workers bodies with well monitored and supervised chelation therapy in hospital.
I can understand that the first example, which didn’t work incidentally, could cause concern. It’s important to limit exposure to lead as much as possible and not bothering to do that is pretty blatant. But I do understand the logic since chelation is a lot less expensive that equipment to minimise lead dust production and exposure.
But medically supervised monitoring and treatment to remove lead? Isn’t that a positive move?
Apparently not. “Routine chelation to prevent increased or reduce current blood lead levels is unacceptable whatever the setting.“.
Okay, so this is a bit like saying we can test for the presence of cancer, but we can only attempt to treat it if it’s stage 4 cancer. Really?
If you read this review article: (Royce S, Rosenberg J: Chelation therapy in workers with lead exposure. West J Med 1993 Apr; 158:372-375), you might start to understand what the nonsense in the OHSA standard is all about. I can’t help pointing out that the authors don’t appear to have understood what they were talking about when it comes to chelation, though that’s fairly common. The comment “Evidence that chelation therapy with edetate calcium disodium is ineffective in treating atherosclerosis led the California Medical Board to consider this practice unacceptable.” While removing lead in a timely fashion may have prevented atherosclerosis, removing calcium plaques from arteries uses the same form of EDTA as treating patients with hypercalcemia, Disodium EDTA. Calcium disodium EDTA will NOT remove any calcium form the body. Surely anyone writing a review about chelation would know that. If they don’t, they shouldn’t be commenting on chelation.
The scary part is this review is used as a basis for decision-making by OHSA. Ignorance feeds ignorance, it seems.
Then “Chelation initially lowers blood lead levels and therefore may decrease the length of time an employee must be away from lead exposure and provided medical removal protection benefits under the OSHA standard. Employers may thus be encouraged to rely on chelation rather than instituting controls to prevent lead exposure.
Treatment using chelation agents represents the failure to prevent lead overexposure and should trigger further follow-up. Physicians caring for workers with elevated blood lead levels can play a key role in identifying others at risk and in prompting actions by workers, employers, and governmental agencies to control lead exposure in workplaces.
This review provides the justification for the latest OHSA standard.
But let’s repeat that statement, “Treatment using chelation agents represents the failure to prevent lead overexposure“. In the context that chelation and the benefits of removal of lead is ignored, this almost makes sense. But in the context that the amount of lead in a lead workers body is constantly increasing to the point where serious symptoms WILL occur, it is utter nonsense.
One last gem: The routine use of chelating agents to prevent rises in blood lead levels or the development of symptoms is considered “prophylactic chelation” by OSHA, which prohibits such practice by any person retained or supervised by lead-using employers, and constitutes inappropriate medical practice.
In the US lead industry, environmental monitoring, blood lead monitoring and removal from lead exposure if overexposure happens, are the ONLY mandated and allowed safety provisions implemented for the safety of lead workers. Workers are treated by chelation only when there is an imminent risk of gross injury including death from excess lead exposure.
We need to put the OHSA standard’s comments about prophylactic chelation into a historical perspective by presenting data that makes a mockery of the present-day standard. I’ve found a 1962 paper (Williams JD, Matthews GA, Judd AW, Oral Calcium Disodium Versenate in Treatment of Lead Poisoning , Br J Ind Med. 1962 Jul; 19(3): 211–215.) This presents a study of the effects of oral calcium disodium EDTA (also called Versenate) in workers suffering lead poisoning. It provides a good review of previous work, but more importantly, it indicates the safety and effectiveness of oral EDTA.
And yet, 60 years later, OHSA have effectively banned chelation for anything but severe lead poisoning because chelation upsets their view of how things should work. ”They follow orders as they were told to and will not allow exceptions”, like the Vogons in “Hitchhikers Guide to the Galaxy”.

This is what we have looking after the safety of lead workers.
It would give me great pleasure to be able to say things were better in Australia, but I’m not sure I can. The existing Australian WHS regulations, while not banning chelation, don’t protect workers from the long-term effects of lead poisoning either. What is it about bureaucracy that can make human lives irrelevant?
I’ve called lead poisoning a silent epidemic, and it’s silent because there is SBA (no that’s not a misspelling) testing of lead in the general population (no-occupational lead exposure) and unless you present with a blood lead level of over 45-70 ug/dl (lower value for children) you will not get treated to remove lead, regardless of the fact that damage due to lead (for example) neurological symptoms, blood pressure increases and so on happen at levels below 10ug/dl.
I would encourage you to read the very short article “Lead Poisoning in the 21st Century: The Silent Epidemic Continues”, (Hanna-Attisha M, Lanphear B, Landrigan P, Am J Public Health. 2018 November; 108(11): 1430). It was written by 3 concerned pediatricians about the situation arising in Flint , Michigan. I should be concentrating on WHS issues, but I can’t help reminding you that lead affects everyone.
I’ll quote a section out of this article:
The consequences are one or two more kids in each classroom with symptoms of attention deficit hyperactivity disorder, 10 or 15 more kids in each school in special education programs, and fewer kids who are truly gifted. A five-point reduction in average IQ caused by widespread exposure to lead will result in a 50% increase in the number of children with IQ scores below 70 and a 50% decrease in the number with IQs higher than 130 and some studies have shown that children exposed to lead are at increased risk for school failure, unemployment, and incarceration.
I’ll display the relevant chart yet again:
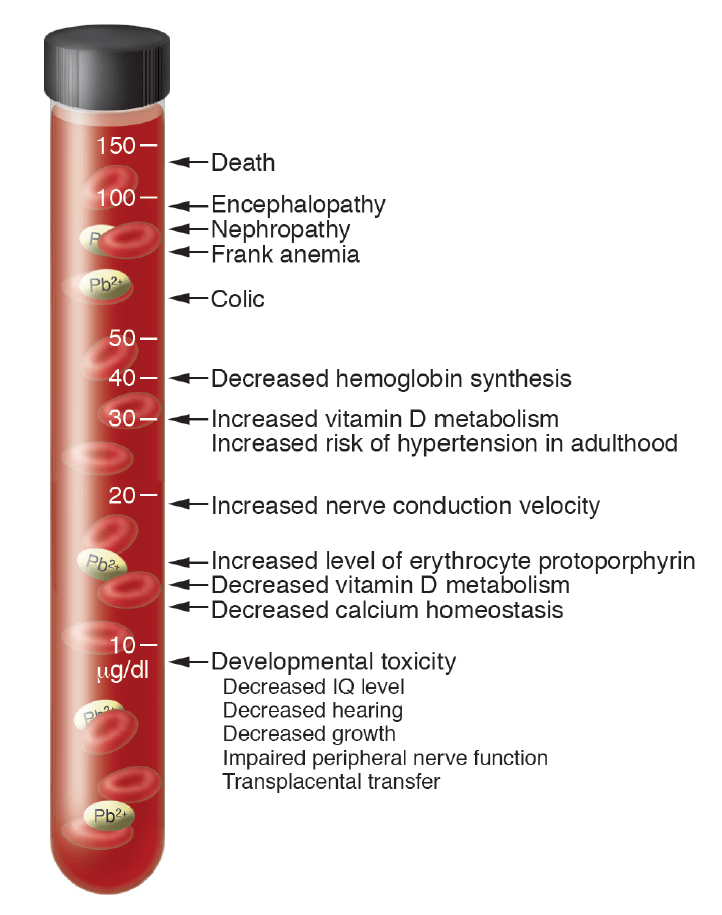
Where do you draw the line and start doing something to halt the inevitable increase in blood lead levels or to remove the lead? How much damage does there have to be before someone takes notice? When are we finally going to redefine what clinical symptoms mean so we avoid this harm?
Our authorities are either dangerously ignorant, or they’re so influenced by the lead industry that they are deliberately ignoring the impact that lead exposure has; the health impact, the educational impact, the impact on our justice system and the overall huge economic cost to Australia.
Sure, we need the mining royalties, but why do ordinary Austrlians have to give up their health and maybe even their lives because of the lack of action about lead.
The inquiry into the Cadia mine dust problems is an example people should consider, as is Queensland Health no longer providing information on notifiable lead tests or the NHMRC recommendation against wide-scale blood lead testing which is so desperately needed so we can properly understand the scope of our epidemic of lead.
One thing is obvious, in the case of both the US and Australia, and that is that occupational health and safety, or workplace health and safety, are not there to ensure a safe work environment for workers when it comes to lead biohazard management. The are there to make sure the often broken rules are enforced. In reading the Safe Work Australia documentation, you can’t avoid the impression that things are more about the employers than the workers, and appearing to be doing something. Since not even the unions that used to be involved in the mining industry have shown any interest in this tragedy of errors, what do we do?.
I wrote that there was an enormous economic cost involved in ignoring lead exposure, and in an earlier post I pointed out the Australia is grouped with other third world counties when it comes to our dependence on mining, and the influence of the miners. We need the money and jobs, and I’m okay with that, as long as people don’t have to give up their health and their lives in the process. We can deal with the dangers of lead if we try. We absolutely have the knowledge and experience to protect people.
But that’s not what happens. Why?
Anyway, scroll down to learn how to protect yourself from lead, because if you don’t protect yourself and your loved ones from the effects of lead, I can assure you that no one else is likely to do it.
