The sad answer is absolutely not, but we have no way of knowing because of the apparent lack of action by so many government agencies.
It is entirely possible, that like the US, Australia is lead poisoned. If we look at the history of lead in Australia, the lack of governmental action with regard to lead exposure in the general population, and the failures in occupational lead safety, this is not an unreasonable conclusion. With less than 1 in 2000 Australians tested for blood lead levels, there is also no credible data to dispute this claim.
There is also evidence of active suppression of information and alteration of safety decisions about lead, and little sign of any proactive action to either recognize or minimise the effects of lead on the population of Australia.
The story of lead in Australia has clear parallels with the much better-known story of asbestos. Just as with asbestos, public authorities were faced with a difficult choice between economic prosperity for the mining industry and safeguarding the health of workers and the public. We know how well that turned out, denial there was a problem until that didn’t work anymore.
I want to add a bit of historical perspective to the comment about active suppression:
Dr Leslie Jon Jarvis Nye was a physician in Brisbane. His 1933 paper in the Australian Medical Journal, “Chronic Nephritis and Lead Poisoning” so concerned the Lead Industry Cartel that they commissioned a “scientific” monograph to refute it.
Although anti-lead paint legislation had been enacted years previously, it was being ignored. With support from the Premier, Forgan-Smith, and the Communist secretary of the Painters’ Union, Dr Nye was able to explain to a meeting of painters the dangers associated with lead paint and from then on, they refused to use it.
I suspect whatever has replaced the lead industry cartel is still unfortunately alive and well. And anyone trying to make the public aware of the dangers of lead might have problems.
If you were living in Australia between 1930 and 2000 you would also have been exposed to the lead from leaded petrol, and that lead continues to contaminate areas near major highways even today. Light aircraft still use leaded petrol so don’t live downwind from a general aviation airport.
Lead paint has been a curse that was recognized since the early 1900s and while high levels of lead were “technically” banned as early as 1922 in Queensland, it continued to be used for another 40years or so. Industrial paints weren’t included in the lead ban in house paints so automotive paint is still available with up to 20% lead.
I would like to quote a 1955 investigation, which found:
“Victorian houses in Queensland characteristically had closed verandas, painted with lead-based paint. Such verandas were ideal for confining small children while their mothers were busy in the house. From daily rain showers in this subtropical region, rain droplets hung on the railings and tasted sweet from dissolved lead. They were within the reach of toddlers, who enjoyed wiping up and licking the rain droplets.”
Renovating pre-1970 houses (some a bit later) painted with lead paint is a huge hazard for the painters, the occupants and any children in the vicinity.
So while the problem of inhaled lead from leaded petrol is now history, the legacy of leaded petrol still remains in the dust in attics, in the soil and anywhere near renovated older houses.
The level of non-occupational lead testing is so low that we have no idea of the magnitude of the problem. I have quoted the 1999 figure of less than 1 in 2000, and can now update this with figures from Medicare (2014) which indicate the testing ratio is no higher. The NHMRC recommended against wide-spread blood lead testing in their 2015 report so the testing ratio is now probably lower. How things have changed.
I would love to be able to state something useful about the degree of risk to the community, especially to our children of historical sources of lead poisoning, but I can’t. Nor can ANY government agency assure us that the dangers of lead are reducing, because without more testing we just don’t know.
But let’s get back on track.
Before I go on, I’d like to point out that there’s a blog post of mine a couple of blogs down from this one that gives hints on how to minimize lead exposure.
Since infants are the most affected by lead exposure, that might be a good place to start in asking a few questions. Here are a couple of incidence maps for autism and ADHD.
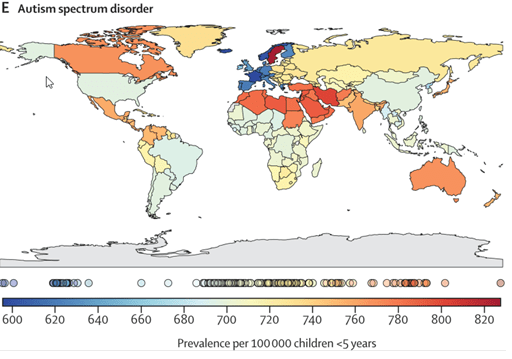
The rate of autism in Australia is about the same as Canada, and a bit more than India. Since this blog post is about lead, I can’t help pointing out that if a baby is exposed to a significant amount of lead, he or she can exhibit autism-like symptoms, and if you’ve read Nancy Hallaway’s e-book you’ll also have realised that at least some of the neurological symptoms can be resolved if the lead is removed.
Considering the opportunities there are for lead exposure in Australia, it would be fair to speculate that at least some of the cases of autism may be caused or contributed to by lead exposure. Something as simple as renovating an old house, sanding off the flaking paint while there are infants nearby, can result in lead poisoning and the symptoms of autism. Living in a lead-rich environment is another scenario where an infant could end up with sub-clinical levels of lead. I use the word sub-clinical because the “clinical” symptoms of lead poisoning are considered to be the ones we’ve known for more than the last century. Oh how this needs to be updated.
There are undoubtedly other causes of autism including genetics BUT one of the possible causes is lead exposure. Why would we not want to filter out those kids and maybe even treat them to reduce the severity of the symptoms? You know, the kids in the older suburb where a lot of houses are being renovated as older people move to retirement villages and younger families have moved in?
Even if the incidence of lead-induced autism was 5%, as an example, that means that 1 in 20 kids with autism could potentially be able to develop normally if they were diagnosed with lead poisoning and treated.
That of course raises two issues, the first that with the exception of children in the lead cities, Broken Hill, Port Pirie and Mt Isa, there is next to no paediatric testing of blood lead levels. And even if the blood lead levels are well above the notifiable limit, the only clinical treatment children will get is chelation therapy IF the blood lead level is above 45ug/dl. Children with non-toxic blood lead levels (less than 45ug/dl) are not treated to remove lead.
That’s a big deal when you think about it. Children with levels of lead known to have harmful neurological effects, do not have the lead removed because they have “sub-clinical” levels of blood lead.
That’s kind of depressing because it’s almost like there is no recognition that lead accumulates in the body. Lead poisoning is subtle, it can be the result of a brief and intense exposure which produces severe clinical symptoms, or something can happen after months and years of lower-level exposure when you’ve accumulated enough lead to produce chronic symptoms or damage to internal organs.
One of the additional challenges to getting treatment for children with sub-clinical levels of blood lead is a widespread belief in clinicians in Australia that chelation is high risk, that it isn’t effective, or that it’s more important to reduce exposure as much as possible.
I know I’ve done this to death already, but it is so WRONG that I need to keep hammering at these misconceptions until people realise that chelation should at least be tried.
The early use of chelation, more than 70 years ago, sometimes resulted in renal failure and death. By the 1960s it was known that the renal failure and subsequent deaths were due to trying to do things too quickly, too high a dose, too often. In fact, it has been found that at much lower doses, EDTA could actually reverse existing renal damage because it acts like an anti-oxidant. IV chelation with EDTA that follows now established protocols does not lead to renal damage or death provided those, safe protocols are followed.
A 5-year old autistic boy died of hypocalcemia during IV chelation therapy. I can’t argue that chelation didn’t kill him, but when I looked up the case, which I thought was due to medical ignorance it turns the pharmacy supplying the EDTA for his chelation therapy prepared a solution of Na EDTA instead of the Ca Na EDTA that had been requested by his paediatrician. Na EDTA is used to treat hypercalcemia because it removes calcium from the blood. Ca Na EDTA is normally used to remove heavy metals like lead because it DOESN’T remove calcium from the body. The child died of hypocalcemia, which caused heart failure. That is an absolute tragedy, a child dying because they were given the wrong drug, the wrong form of EDTA.
But another tragedy has been the many children that maybe could have been helped, that weren’t because of the wide held “belief” that a child can die from chelation therapy because of this incident.
Ca Na EDTA does bind other heavy metals besides lead, like arsenic, cadmium and mercury. As I’ve said before, that’s a bonus, but it also binds zinc and magnesium, which are essential metals. One of the important adjuncts to chelation therapy is trace metal supplementation.
It’s worth mentioning that another use for Na EDTA, beside treating hypercalcemia, is to remove calcium plaques (atherosclerosis). It works quite effectively, though it has to be accompanied post-treatment with trace metals plus calcium. A sad example of chelation therapy being badly understood is that the California Medical board banned the use of Ca Na EDT because it was ineffective at treating atherosclerosis (removing calcium).
Administered with appropriate protocols and caution, IV chelation therapy has been proven to be safe. If it was so dangerous, why do they use IV chelation therapy on children with severe (over 45ug/dl and encephalopathy) lead poisoning? And use an oral chelator if encephalopathy isn’t apparent.
Another argument against chelation therapy is that it isn’t effective because blood lead levels “rebound” after chelation.
When lead is absorbed, most of it ends up in the bones. This varies from about 75% in children to 95% in adults. The lead in bones is in balance with lead in the blood and soft tissues. When a chelator is administered, it binds the easily accessible lead in the blood and soft tissues. If the chelation therapy doesn’t go on for long enough (most treatments are for 5 days) then very little bone lead is removed. Once chelation stops, a new balance between bone lead and blood/soft tissue lead is established, and blood lead levels go back up to a level that reflects bone and body lead levels. A rebound simply means you didn’t remove all the bone lead, not that chelation doesn’t work.
I’d like to quote the first sentence of the acknowledgemnt in the book “Brush with Death” by Chritian Warren:
Writing acknowledgements is similar to receiving treatment for lead absorption: a single course of therapy is supposed to abate a burden that had accumulated over many years. The patient feels better, some of the burden is lifted, but the bulk remains forever bound up in the bone.
Removing bone lead is a case of slow and steady lead removal, with a dose of chelator that is low enough to be absolutely safe, over many months until ALL the lead is gone.
I’m not going to argue that reducing exposure isn’t critically important, because it is. Successful campaigns to reduce lead exposure, for example in Broken Hill, have absolutely resulted in a lower mean blood lead level in children. It would be wonderful if exposure could be reduced to zero, but that’s pretty unlikely. The basic problem with relying solely on the prevention of lead exposure is that there are so many possible sources of lead, that it will at best only ever be a partial solution. Whatever lead is absorbed, will increase the body lead burden, and increase the risk of disease.
The lead that has been absorbed, that is stored in bone, is going to be there, and will keep increasing, unless we can do something about removing it. Diet can play a significant role is reducing absorption of lead, some food ingredients like citric acid are weak chelators, so in the absence of lead exposure, an appropriate diet could gradually reduce body lead levels.
But if you want to remove lead in something less than decades, using a chelator that is reasonably specific for lead is a pretty good move.
I’ve talked about this before, but I think this is the right place to bring it up again. Cattle in far North Queensland graze on land that has naturally occurring lead deposits (not due to pollution from mining/smelting) and they have high enough lead levels that they have (recently) been found to be unfit for consumption. Some smarter than average station owners use a chelation agent which is used to remove heavy metals from flue gases, TMT 15, to remove lead from the cattle, and make them fit for consumption. TMT has such a high affinity for lead that it can remove all the lead from the cattle in a few weeks. I wouldn’t use TMT 15 on humans because it hasn’t been tested on humans as far as I know, but if we can remove lead from the cattle we eat, why can’t we remove lead from our children, and ourselves.
But there’s a bit more to the story I suspect.
I’ve just read an article in “The Conversation” (https://theconversation.com/lead-poisoning-of-port-pirie-children-a-long-history-of-looking-the-other-way-8296#:~:text=Port%20Pirie%20has%20been%20affected,poisoning%20was%20fine%20lead%20dust.). The title is “Lead poisoning of Port Pirie children: a long history of looking the other way”.
I’m going to quote the beginning of the article:
It is shocking to discover that more than 3000 children have been lead poisoned in the South Australian town of Port Pirie during the last decade.”
Whilst Australia continues to be a world leader in lead mining, smelting, and processing, the adverse impacts associated with production have been consistently downplayed by industry, governments, councils, health officials, and regulators. Even some academics argue the effects of low lead exposures are not of significant concern. Due to ignorance, misinformation, and deliberate obfuscation of evidence, generations of families living next to lead-mining, smelting, and refining centres such as those in Broken Hill, Port Pirie, and Mount Isa, have been and continue to be exposed to environmental lead, a known neuro-toxic contaminant.
More than a century of IQ-lowering poisoning continues
Childhood exposure to lead has been linked to lower IQ and academic achievement, and to a range of socio-behavioural problems such as attention deficit hyperactivity disorder (ADHD), learning difficulties, oppositional/conduct disorders, and delinquency. The disabling mental health issues from lead exposure often persist into adolescence and adulthood.
There’s a lot more and I would encourage you to read the whole article. While Mt Isa has only had a lead smelter for a bit over 90 years, it is unlikely that there has been any less lead pollution, except perhaps in the last 15-20 years.
I guess the point I’ve drawn from the Port Pirie example is pretty obvious in the title in the Conversation article, ”a long history of looking the other way“. That’s what Queensland Health (QH) have been doing for at least the last decade, possibly longer. I don’t mean the whole organization because I know there are people in QH that are deeply concerned about lead in children, but apparently not the bureaucrats.
I am pleased to have found out there is serendipitous testing of blood lead levels in children in Mt Isa. When blood sample are taken from children in the Mt Isa hospital, any excess blood in the sample is tested for lead. If high (greater than 45ug/dl) levels of blood lead are detected in children , they are treated to remove excess lead. Lower levels of blood lead result in activities to minimise lead exposure, but no treatment to remove lead. This is despite a huge amount of clinical and epidemiological data that blood lead levels as low as 5-10 ug/dl can have serious neurological consequences.
There is voluntary testing available for adults in Mt Isa (and children, though infrequently). In adults, anything under 75ug/dl is again untreated, despite evidence (some shown below) that blood lead levels over 5-10ug/dl can increase the risk of death due to cardiovascular disease.
The next incidence chart shows something even more disturbing about Australian children.

As you can see on the world map, Australia is in a class of it’s own when it comes to ADHD incidence. The causes of this disproportionately high rate of ADHD are probably due to a lot of things, like still using insecticides, fungicides and other chemicals banned in most other non-third world counties. One of the causes could be toxic metals which are far more prevalent than we realise.
ADHD is attention deficit hyperactivity disorder. It’s a neurodevelopmental condition that is characterized by developmentally inappropriate levels of inattention, impulsivity, and hyperactivity that can cause a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development.
For a long time, clinicians thought you grew out of ADHD, but it turns out that isn’t the case because while many adults and young adults with ADHD have compensated to live fairly “normal” lives for some it has resulted in severe functional, social or occupational impairment.
We have no idea why Australia leads the world in ADHD incidence, but I do know one possible contributing cause, lead. Just like the scenario where lead exposure can cause something that looks like autism, it can also cause symptoms of ADHD. But do we test for lead exposure if ADHD is suspected?
In Australia, we treat ADHD with drugs. The psychostimulant medications mainly used to treat ADHD are dexamfetamine, Ritalin and lisdexamfetamine. These drugs have a bucket-load of potentially severe side-affects like psychoses, mood swings and even seizures, so there is significant risk involved. They also need to be taken long-term as they are not a cure.
IF some of the cases of infant ADHD are caused by lead, and removal of the lead provided a permanent cure, that would be worth doing. Why don’t we measure blood lead levels to find out, and is chelation really more risky than psychoactive drugs where we have no idea of the other possible consequences?
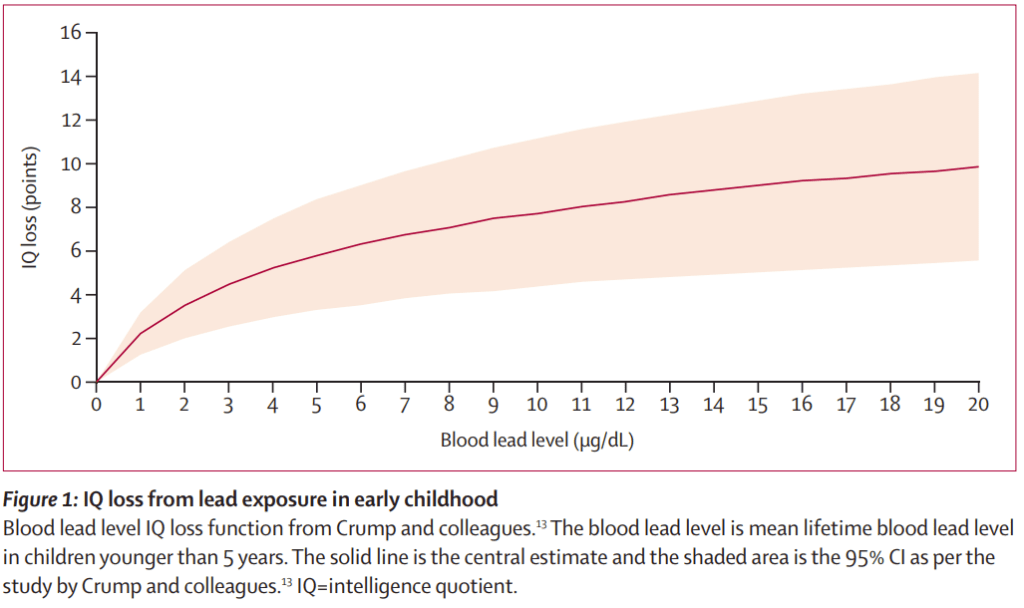
How about the other not so obvious effects of lead on infants, like a drop in IQ? I’ve shown the graph of IQ loss vs blood lead levels in an earlier blog, but here it is again (from the Lancet):
It’s hard to be more eloquent than the following article in the American Journal of Pediatric Health. I’d like to quote the complete article because it’s short and so well worth reading.
Lead Poisoning in the 21st Century: The Silent Epidemic Continues
Creating a disturbing sense of deja vu and in line with current trends of science denial, some skeptics are seeking to minimize the Flint,Michigan, water crisis and thus impede efforts to mitigate this humanmade disaster and prevent similar crises. They argue that the rise in Flint children’s blood lead levels did not warrant a state of emergency and that Flint’s kids were not poisoned. They are wrong. We represent three generations of pediatricians and child health researchers. In our professional lifetimes, we have seen repeated reductions in the levels of lead considered toxic as new research has shown time and again that blood lead levels previously considered safe are in fact harmful to children’s health. With each of these reductions, we have battled waves of skepticism from well-meaning academicians, the inertia of government agencies, and nefarious attempts by industry and their agents to undermine the science and to dismiss the increasingly clear evidence of lead’s toxic effects at ever lower levels. The science is now unequivocal. There is no acceptable level of lead. There is no safe threshold. Lead is pernicious at the lowest increments of exposure. The World Health Organization and the Centers for Disease Control and Prevention have declared that no level of lead in blood is safe. Driven by austerity and a corrosion of democracy, Flint’s public health disaster resulted in population-wide lead contamination of drinking water. In many homes it was categorized as hazardous waste. Not surprisingly, people interpret ingesting a poison as being poisoned. This definition of poisoning may not be equivalent to the toxicologist’s definition of acute poisoning, but it is poisoning and its consequences can be lifelong. This semantic nit-picking is counterproductive. There should be no disconnect between doctors who treat individual patients and public health practitioners who look at population-wide data and implications. Today, children rarely come to our emergency departments and intensive care units with symptoms of acute lead intoxication—seizing and being comatose—as they often did in generations past. However, this does not equate to no harm done. The impact of lead is insidious and often referred to as a “silent epidemic.” The effects of lead poisoning are not usually detected in a short visit with a doctor. The population impacts are, however, staggering. The consequences are one or two more kids in each classroom with symptoms of attention deficit hyperactivity disorder, 10 or 15 more kids in each school in special education programs, and fewer kids who are truly gifted. A five-point reduction in average IQ caused by widespread exposure to lead will result in a 50% increase in the number of children with IQ scores below 70 and a 50% decrease in the number with IQs higher than 130. In adults, lead exposure results in cardiovascular and kidney problems. And some studies have shown that children exposed to lead are at increased risk for school failure, unemployment, and incarceration. Now more than ever, it’s time to renew and refocus efforts to ensure that the blood of children in cities such as Flint; Detroit, Michigan; Chicago, Illinois; Baltimore, Maryland; Newark, New Jersey; Philadelphia, Pennsylvania; and beyond are never used as detectors of environmental contamination. Specifically, this means a renewed effort to update outdated action levels, remediate homes, replace lead pipes, and eliminate all the other sources of lead in our environment before our children are poisoned. That is the legacy we hope to leave the next generation.
Australia may not have a Flint Michigan where incompetent officialdom stupidly poisoned much of a small city with lead because of lead leaching out of lead pipes, but we do have areas of cities that have high levels of lead, either as a result of leaded petrol, or environmental lead, or lead pollution from the mining, smelting and transport of lead.
And we have a lot of government agencies that are pretty busy ignoring the true cost of ignoring lead poisoning. And there was the situation in Yarrabah where a broken-down pH adjuster allowed acidic bore water to leach lead out of brass fittings and lead soldered pipes. When various news services had headlines about lead poisoning in Yarrabah, the Health Minister went there to announce funding for a new pH adjuster. That was one year after the request for funding for a replacement, but it’s pretty obvious that in the absence of politically damaging news stories, it’s easier to ignore any problems.
Thanks to lead paint and a host of other sources of lead, I can state with absolute certainty that some children in Australia will be adveresely affected by lead and have their futures blighted. Let’s make a guess about how many.
There are roughly 1.5 million children aged under 4 years in Australia who are exquisitely sensitive to lead, 2.2 million between 5 and 12 and 1.4 million between 13 to 17. The US has the added risk of lead pipes in older houses, so statistics of 1 in 6 children affected by lead quoted by the CDC may possibly overestimate the number of children affected in Australia. But even if 1 in 20 children are affected by lead in Australia, that equates to about 250,000 children in Australia that are potentially affected by lead. It’s anyone’s guess if this is the case because we just don’t know thanks to the lack of testing. Talk about looking the other way!
We have all the rest of the sources of lead exposure that are seen in the USA. But there is a big difference in one area. With the possible exception of Broken Hill, there is little evidence that any government agencies are taking any active steps to drastically reduce lead exposure. It’s notable that in Broken Hill the lead exposure reductions have largely been due to local community action.
I guess it’s now time to focus on adults.
Let’s start with another graph posted earlier from the Lancet. This is cardiovascular death risks versus blood lead levels.
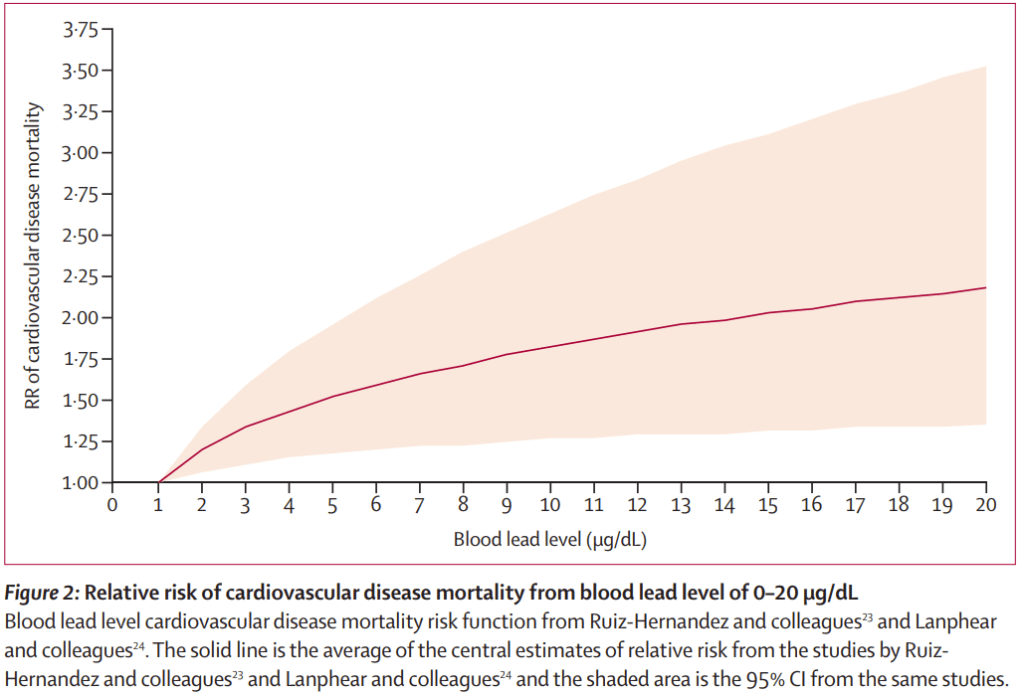
Notice that anything over 1 ug/dl results in an increase in the risk of death from cardiovascular disease, whether it’s atherosclerosis, peripheral vascular disease, high blood pressure causing strokes and so on.
Long term studies of the health of lead risk workers in Australia has found alarming increases in the incidence of various cancers in workers exposed to lead. As for the general population, we don’t know because just about the only people that get tested for lead are people whose occupation exposes them to lead.
If we don’t test for lead in the general population, then the authorities can also “safely” ignore the effects of lead on the general population. It doesn’t mean that people aren’t adversely affected by lead, but by not testing them, we simply don’t know. If our governments are unwilling to acknowledge the costs to our economy of doing nothing about lead, then we have a problem.
If we add up the health costs: the costs to the justice system, the loss of wages, the social costs of supporting lead-affected children, the reductions in productivity due to loss of IQ, and the economic costs of deaths caused by lead, the total amounts are enormous. And yet we (our government), continue to look the other way when it comes to lead. Are they so corrupt and influenced by lobby groups, or are they afraid to open the Pandora’s box of damage that lead inflicts on the community?
There’s really not that much more to say that hasn’t been said already. But it would be remiss of me not to point out that youth and adult violence and crime have been linked to lead exposure. The next time you hear about demands for more policing to reduce crime, maybe some blood lead testing could reveal a problem that might have a solution other than more youth detention centres.
