I thought I’d say a bit more about the workplace health and safety (WHS) processes for lead risk workers and what the health department doesn’t do for children exposed to lead. What prompted this was a picture I found on social media about mine canaries.
As you know, canaries used to be taken down into coal mines because they would be affected by poison gases before the miners. If the canary fell off his perch, then it was time to get out of the mine. That seems a bit hard on the canaries and despite the horrible working conditions for miners in a coal mine, they made this:
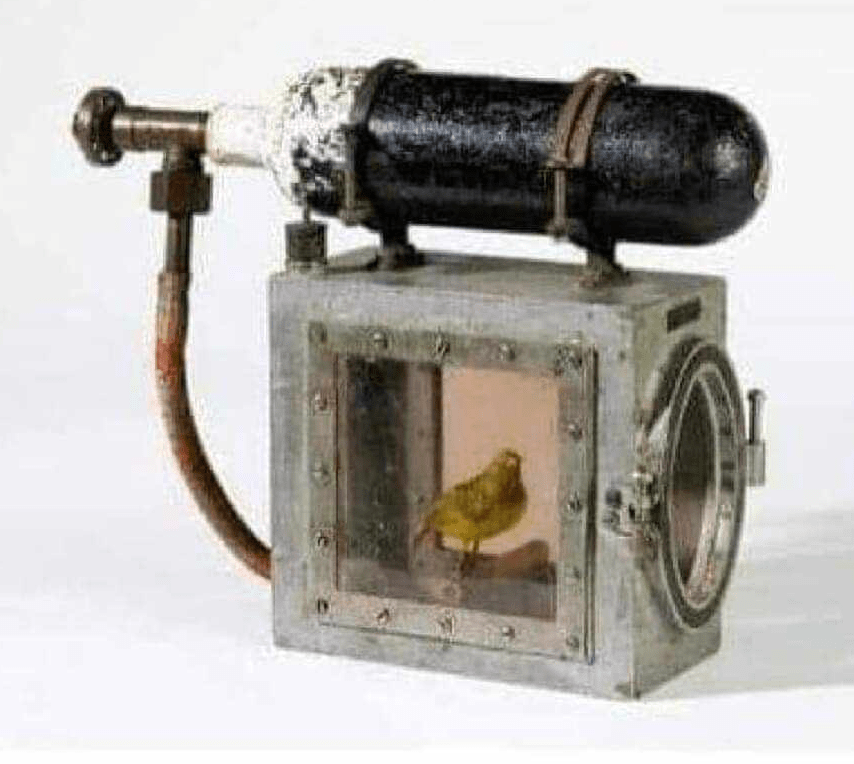
The cylinder has an oxygen tank and if the canary fell off his perch, the glass door would be closed and the oxygen turned on to revive the canary and keep it alive while the miners left the mine with the canary.
The miners cared enough for the life of a small bird that was protecting their lives, to value its life and keep it alive.
I’d like to talk about two situations where people exposed to lead are used in a way similar to mine canaries, except perhaps that their lives aren’t valued as much.
The first situation is the one faced by lead risk workers, people exposed to lead in their occupations, their jobs. I have a earlier blog that talks about lead risk workers, though I have to be realistic and point out that some of them aren’t monitored for blood lead levels, people like soldiers for example. But let’s go on.
If only the WHS authorities and employers were half as caring about lead risk workers as the miners about their canaries. Or perhaps update their decades-old regulations that indicate they really don’t care.
Lead risk workers are their own mine canaries from the viewpoint that if by accident, bad hygiene or increased lead pollution their blood lead levels (BLL) increase above the actionable limit, the excess BLL is an indication of some sort of lead exposure failure. That is supposed to trigger some sort of investigation and remedial action, but more often than not it doesn’t. Things go on as usual.
If your BLL goes above 30ug/dl, you are removed from the lead risk, and your BLL is monitored, and once your BLL drops below 20ug/dl you can return to the lead risk work because the lead is gone.
If the fall in BLL truly indicated a drop in body lead levels, that would be a perfectly reasonable thing to do, except we’ve known for the last 40 odd years that it doesn’t. BLL falls because red blood cells containing lead are cleared from the body, most of the rest of the lead goes to your soft tissues and then your bones.
Unlike the canary, removing you from lead risk work doesn’t remove the lead you’ve absorbed, you don’t end up safe until the next time. Lead accumulates in your body and once the lead levels get high enough, they will result in all sorts of harm.
The sad truth is when you go back to work, you will continue to accumulate more lead.
So is anything done to protect you from the ill effects of lead, like the oxygen fed to the canary?
NO!
If your BLL goes above 70ug/dl, you will get a relatively short course of a medical treatment, chelation therapy, to drop your BLL back down to “safe” levels. If you’ve accumulated a lot of lead, once the chelation therapy has stopped, a few weeks later your BLL will go back up, because of lead released from your bones This is called rebound and for the most part, clinicians don’t understand why it happens because they know so little about the toxicokinetics of bone lead. There’s an interesting article in Environmental Health Perspectives, Vol 91, pp 33-37, 1991 by MB Rabinovitz that makes sense of the active distribution of lead between the bones and soft tissues in the body. Notice the date, 1991, 33 years ago!
Unless a low dose, long term chelation protocol is used, lead cannot be effectively removed from the bones, or the body.
If your BLL goes over 30ug/dl, there are a multitude of risks that start to climb astronomically, like the risk of soft esophageal cancer, cardiovascular death, behavioural changes, violence and so on.
Nothing is being done in Queensland, or indeed in Australia, to reduce these risks.
NOTHING!
In an ideal world we would have environmental monitoring of the workplace to detect excess lead hazards, BLL monitoring combined with measurement of bone levels, and chelation to remove accumulated lead, and to stop it accumulating.
That’s something that could be done right now, but the WHS authorities or employers aren’t interested in changing what they are doing, because they would then be legally aware of the workers’ risks, and that could have unfortunate consequences, including having to spend money to make the workplace safer.
The second situation I’m going to describe is in a lot of ways worse.
Children get exposed to lead, by eating or licking lead paint, by environmental exposure, old batteries and other sources of lead, like lead from eating a wild duck, shot by a hunter.
With the exception of children in Australia’s lead cities, Broken Hill, Port Pirie and Mt Isa, children rarely have their BLL measured unless they are showing overt signs of lead exposure. I’d like to point out that the symptoms used to diagnose overt lead exposure are the ones used 60 years ago, before evidence was available that much lower levels of BLL indicated harm.
If a child’s BLL is above 45ug/dl. they will be treated with chelation therapy, either with IV chelation (Ca Na EDTA) if encephalopathy is evident, or with oral DMSA (dimercaptosuccinic acid). Either type of treatment is generally short-term and discontinued once the BLL drops to what is considered safer levels. Of course that’s ignoring the American CDC, who has dropped the recommended maximum level to 3.5ug/dl but also states there are no safe levels of lead in children.
If the child has been chronically exposed to lead, several weeks after the chelation therapy their BLL will increase, a rebound, due to the release of lead from bone. The rebound has been described as indicating the failure of the effectiveness of chelation. Chelation is generally not continued because of the mistaken belief it is risky.
In any event, children with a BLL below 45 ug/dl generally receive no treatment. Their parents are counselled, sometimes with a site inspection, to reduce exposure to lead, ideally that includes nutritional counselling which can make a big difference for children.
But most of the lead in their bodies remains. We now know that relatively low levels of lead, below 10ug/dl, can have major deleterious neurological effects. But nothing is done to remove the harmful lead.
We also know that any amount of lead in the body is potentially harmful, but our medical authorities do nothing. We know that BLL levels of 10ug/dl can lead to a drop in IQ, in severe educational challenges, and also lead to behavioural changes that can manifest themselves as violence in older children, but our medical and educational authorities do nothing.
These children are the mine canaries for lead exposure, an indicator of excess lead in the environment. But they get no “oxygen” when they start to succumb to the effects of lead. They are simply discarded as faulty.
The government agencies that we are supposed to be able to trust, ignore their duty of care and look the other way, whether because of ignorance, laziness or corruption. In this scenario my definition of corruption has to be pretty broad, because a government as a whole can be so influenced by mining interests, historically the lead industry cartel, that the “unofficial” line for public servants is to look the other way. And sometimes, it can be because the government fears the results of the public finally finding out about their long-term failures to control environmental hazards. Think about asbestos if you don’t think that’s possible.
The really sad joke about all this activity to hide the effects of lead exposure is that we now have the means to protect workers and children from the ill effects of lead absorption and accumulation. But in order to move forward, we have to admit our past failings. Bureaucrats hate admitting they were wrong, it’s simply not in their genes to admit fault UNLESS they’re caught out.
So here we are. We know there’s a problem, we know about the solutions, and as far as Queensland is concerned, we do nothing. Makes you proud to be a Queenslander doesn’t it?
