I took the time to go through a 2016 Safe Work Australia (SWA) document which described the decision and consultation process that went into changing existing workplace health and safety rules.
After a lot of reading, I found things weren’t nearly as bad as I’ve previously stated, and in some instances they were worse.
Having read quite a few of the US Occupational Health and Safety (OHSA) documents, I now have a much better understanding that the OHSA regulations form the foundation of SWA model regulations referring to lead.
The SWA consultation process is much more comprehensive than I had thought. It involves proposing several different incremental change options, together with a cost/benefit analysis of the results of the proposed options.
Provided the cost/benefit analysis is acceptable to a majority of employers, a progressive (enhanced safety) change may be rolled out, generally with 2-4 years for implementation.
That sounds a lot better than my earlier claims that employers could effectively veto changes, but it does basically amount to the same thing. What I had failed to understand is that the number of WHS claims, and their value is also used when considering the viability of regulation change options.
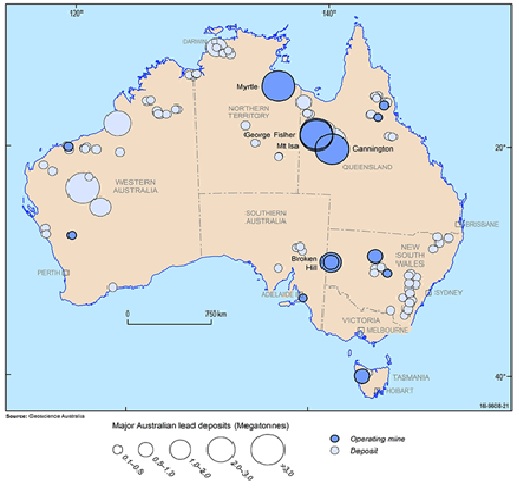
One thing that was made clear is that the SWA model regulations weren’t absolute. That is, if an employer wanted to implement more stringent safety procedures, they were free to do so. The SWA model regulations are not a straitjacket, they’re a guide for minimum acceptable standards. That said, the more progressive and safety conscious employers didn’t include companies like Glencore who is the biggest lead risk employer in Australia.
But the main stumbling block is still the use of blood lead levels (BLL) as decision points in dealing with safety issues. One of the 2016 option tradeoffs was that if lower BLL levels were accepted, then the frequency of blood lead testing could be reduced.
I’d like to take this opportunity to explain why less frequent BLL testing makes using BLL even more pointless.
I came across an interesting quote: “Due to the short half-life of lead in the bloodstream, BLL cannot be used to diagnose or rule out evidence of exposure that occurred more than six weeks prior to testing.” (Philip AT, Gerson B. Lead poisoning – Part II. Effects and assay. Clin Lab Med 1994 Sep;14(3):651-70,).
Why does this matter? What it basically implies is that unless you are measuring BLL at no more than monthly intervals, you can’t be sure of what you’re measuring when it comes to lead exposure. Lead accumulates in the body, in the bones, and the existing lead in your bones contributes to whatever lead is in your circulation due to exposure. BLL, as is used in the occupational sense to make decisions about safety, simply doesn’t measure up as any sort of indicator.
It’s worth taking this a bit further. The executive summary of the SWA document on the health effects of lead (https://www.safeworkaustralia.gov.au/system/files/documents/1702/review-hazards-health-effects-inorganic-lead-report.pdf) makes some statements that I’d like to dissect after the sentence that states the health effects of lead are directly related to the concentration of lead in the affected organ systems:
This in turn is directly proportional to whole blood concentrations. Blood lead (PbB) concentrations have been the traditional measurement of internal exposures to lead and indicators for management actions for persons overexposed to lead in the workplace.
Blood lead is a measure of the amount of lead in whole blood, red blood cells and plasma. Red blood cells bind lead and in acute lead exposure represent up to 98% of the lead in the blood. Plasma lead only makes up about 2%.
However this picture changes markedly when exposure has been chronic. In that scenario, the proportion of blood lead in plasma is much higher, largely due to the release of accumulated lead from bone. This means we have 2 significant pools of lead in blood; lead in red blood cells which fluctuates up and down depending on current exposure and breakdown of red blood cells, and reasonably constant but ever-increasing contribution of lead that has been accumulated in the bones.
Are you willing to guess what is actually being measured?
While things are obviously not terribly precise in any which way, you’d think the outcome of overwhelming evidence to the contrary was force some change.
The problem is that changes in Australian WHS rules relating to lead are infrequent (5-10 years) and there appears to be no urgent moves to update the model regulations to implement something like XRF to accurately monitor health risk and using chelation for prophylaxis lead lead exposure risk management..
“Proper” environmental monitoring of lead dust and fumes in the workplace could replace BLL with something far more accurate and timely. The only things environmental monitoring couldn’t do is manage scenarios such as taking off dust masks because the ambient temperature is 50+ degrees, or too crowded or too dirty change rooms, but it would provide a far better indication of excess exposure.
Then again, if dust mask filters were analysed for lead content, that could achieve two things, personal environmental monitoring, and detection of non-compliance in wearing PPE.
Then again even if accurate monitoring of exposure were possible, we’re still left with the problem that unless lead exposure can be reduced to nothing, workers will still accumulate lead in their bodies.
But if you can stop lead being absorbed and remove existing lead from a lead risk workers body, lead ceases to be the long-term danger that it was. Chelation is used as a last resort treatment in the face of dangerously high blood lead levels. That requires an IV infusion of chelating agent, a proper clinic environment, nurses etc.
Oral chelation could be a game changer, because it requires no or minimal medical supervision, is inexpensive and safe. It was first used in the early 1960s to effectively slow lead uptakes and remove lead from the body. However it had two drawbacks, it “interfered” with the moniotring of lead exposure and was used by some unscrupulous employers as a way to avoid having to clean up the working environment to reduce lead exposure. As a result the US OHSA saw chelation not as a way to protect worker’s health, but an intolerable nuisance which interfered in the management of lead exposure. “Safety” has to be able to be monitored and quantified regardless of a worker’s health outcomes.
An oral chelator for lead has to be reasonably specific for lead, freely available without prescription, and safe over a wide range of dosages. The calcium disodium salt of ethylene diamine tetra acetic acid (EDTA) fits these criteria. It’s a registered food additive, (#385) which works by preventing oxidative (metal catalyzed) damage of food stuffs, something it does quite well in the body as well. There is no regulatory barrier to it’s use in food, as an example provided the maximum daily dose is 2.5mg/kg body weight which is based on a 100-fold safety margin.
Considering all the detrimental effects of even low levels of lead in the body, chelation seems like a no brainer, except that EDTA has somehow managed to gain a bad reputation in medical circles in the western world.
The most common comments are: chelation is dangerous and can cause death and renal damage, and chelation was responsible for the death of a 5-year-old child. These comments are true for IV Sodium EDTA infusion at high dose and duration, something that hasn’t happened for the last 40 years once safe treatment protocols were established. The 5-year-old child died from the IV infusion of the wrong form of EDTA supplied due to a pharmacy error. Disodium EDTA was supplied despite calcium disodium EDTA being requested. Disodium EDTA can cause hypocalcemia, calcium disodium EDTA can’t. The child died of hypocalcemia.
If WHS procedures were truly interested in worker safety, then monitoring lead accumulation in the body, and managing lead accumulation (and removal) with oral calcium disodium EDTA would deliver the desired result, safe workers unaffected by lead exposure, particularly if this was combined with environmental monitoring to reduce lead exposure. But WHS isn’t about ensuring worker safety when it comes to protecting them from the multitude of health issues resulting from excess lead accumulation.
That has to change.
While XRF spectrometers for diagnostic use are quite expensive, so is the amount of money paid out in claims, and claims settled out of court (with NDAs). Oral chelator sufficient to stop lead accumulation in the body and gain net removal of lead would cost under 10 cents a day. That’s the cost of keeping lead risk workers healthy.