That’s a somewhat controversial title for this post. Where lead exposure “safety” is concerned, my opinion is they’re not doing their job. But that statement requires clarification.
We have a regulatory body for workplace health and safety that develops regulatory models for the states and territories of Australia (except Victoria). This is what Safe Work Australia (SWA) say about their role:
Safe Work Australia is a national policy body representing the interests of the Commonwealth, states and territories, as well as workers and employers. We work to achieve healthier, safer and more productive workplaces through improvements to work health and safety ( WHS ) and workers’ compensation arrangements.
When SWA formulates regulations about workplace health and safety issues, it is a complex process of introducing amended rules, discussion and then deciding whether the changes are justified, much like parliament, where the people with primary voting and indeed veto rights are the employers , and representatives of employers and government agencies. While workers are allegedly represented I have found no evidence of direct worker consultation or representation.
When you look at the decision-making process around lead biohazard management, as an example dear to my heart, there is no evidence that worker safety had any sort of precedence.
Lead exposure management regulations have remained unchanged for over four decades, with the exception of the lowering of the trigger blood lead values for work removal and resumption. This is despite an overwhelming amount of clinical and epidemiological evidence that indicates the basic premise of these actions is incorrect. It is despite the fact that SWA’s own publicly accessible documentation very clearly indicates the basic premise of the regulation is simply wrong.
And yet they continue this abomination in their regulatory model because it best suits the employers. If you know you’re doing harm, what does that say about an organization that refuses to consider change?
I’d like to present an email I sent to the SWA Chemical Policies director after getting a reply that basically did what bureaucrats do, repeat what the organization does instead of answering any specific questions.
Here it is:
I have to apologise for bothering you again, but I have had a prior issue around lead exposure management in lead risk workers that I tried to raise with SWA.
I was pretty naïve at the time, not having any experience with the workplace health and safety mantras, and not understanding how safety had to be cost-acceptable when proposing updated safety regulations.
You would be aware of the fact that lead exposure monitoring and management achieves nothing but excess lead exposure detection , and only IF the employer sees rising blood lead level (BLL) as a failure of exposure limiting processes and does something about it.
I have second-hand information about lead risk workers removing their dust masks because of 50 degree heat, with their faces running with black sweat and of change rooms that were too crowded with lead dust on the floor.
If rising BLL is used as an indicator of degrading environmental safety, or unacceptable worker habits or actions, and as a trigger for investigation and rectification, then I acknowledge its value in exposure monitoring and management.
But nothing is done about the continued bioaccumulation of lead.
SWA documentation makes it pretty clear that whoever composed the document on lead knew about lead bioaccumulation and the very long half-life of lead in bone, as well as the fact that most lead ends up in bone.
But aside from a reference to how x-ray fluorescence (XFR) spectrometry could possibly be used to measure bone lead and saying XRF wasn’t ready yet (2019), SWA has no alternative to measuring BLL, doing what they’ve been doing for decades, with the occasional adjustment of the trigger levels (now 30ug/dl and 20ug/dl). I would like to provide an update (enclosed) where work by Linda Nie’s group at Purdue University now has portable XRF measurement of bone lead at a point where it can and should be used.
If we don’t measure bone lead and by extension body lead levels, we remain unable to even attempt to manage lead worker’s ever increasing body lead burdens, which WILL cause disease in the future, if not already.
A long-term Monash study of lead workers, mentioned in a SWA document, notes a 7-times higher rate of oesophageal cancer in workers with a BLL of 30ug/dl. When a worker leaves lead risk work, they have a 2-3 fold higher risk of dying of cardiovascular disease at a BLL of 15ug/dl. We also have gout, high blood pressure, atherosclerosis and a host of other conditions.
SWA knows about this and effectively ignores it as far as the current regulation model is concerned. Lead risk workers’ have a real risk of developing serious disease or death because the true dangers of their lead risk work, aren’t properly addressed.
I accept that any effective way of reducing the bioaccumulation of lead (an inevitable result of exposure) is worth doing, but it ignores the result of the bioaccumulation.
I’ve neglected the truly devastating effects to children of mothers who have worked as lead risk workers. Lead, like calcium is removed from the body during gestation and during breast feeding.
Doing nothing about managing a worker’s body lead burden can have devastating consequences.
Even if XRF finds it’s way into the model regulations, we are still left with the problem of what to do about the already accumulated lead. Chelation or removal of lead provides a remarkably elegant solution, provided we stick to oral chelators.
I need to point out the US OHSA explicitly forbids using “prophylactic” chelation to remove lead since it interferes with BLL measurements and confuses the results of monitoring. I would like to argue that removing lead that is already present is not prophylactic, but I don’t have the proper bureaucratic mindset.
Nevertheless, the inescapable truth is that if we know the body lead burden of a worker using XRF, and we are hopefully minimising exposure using BLL, we still need to manage body lead levels either by preventing lead being absorbed at all, or by removing it.
Cattle in far north Queensland live on land that is rich in natural lead. As a result they end up having so much lead in their bodies that they are now unfit for human consumption. A few weeks in a feedlot eating an industrial chelating agent leaves them lead-free and fir for consumption.
The station owners needed to produce a cost-effective solution to make their cattle saleable, and they found one. Is it really too hard to look at this for lead-risk workers?
I’ve managed to get a few lead risk workers to volunteer for a trial of 600 mg Ca Na EDTA in an enteric capsule (cost 13 cents per capsule, with occasional trace metal supplementation) daily. The sample size is too small to be meaningful, but what we are seeing is a steady fall in BLL, in spite of continued exposure to lead. The first time something like this was reported was in 1962, so I’m simply repeating something already done 60 years ago, albeit at a much lower dosage (they used 4g Ca Na EDTA daily).
My logic was that it takes time to remove bone lead, so slow and steady minimised any risk, and was probably going to be more effective. I guess we’ll see.
Removing lead with oral chelators is not a new idea. But it’s high time it was considered as a tool to make sure that lead risk workers didn’t carry an awful legacy from their work, all while they were under the protective umbrella of SWA or their state WHS organizations.
I am aware that part of the decision process for formulating updated (and perhaps safer) model regulation is cost-driven, namely the cost of implementation and employers can argue against changes that are deemed to be too costly. In a proper cost-benefit analysis, a costing has to be included for the costs of NOT changing the regulations.
I’m sure you wouldn’t be surprised to learn that I didn’t receive an answer. That’s par for the course when a bureaucrat doesn’t want to answer an awkward question. Ignore it and it will go away.
I’ve talked about the constraints on people in organisations about communication, how hard it is to be a whistleblower and the likely outcomes of speaking up. We know what happens to whistleblowers in Australia and what it says about the claimed openness of our governments agencies.
Nevertheless, it was disappointing, because if SWA as an organization cares more about employer opinions than worker safety, they aren’t doing their stated job. I understand that safety regulations that are too expensive can affect the viability of an industry and unemployed workers aren’t that well off either. When invoking updated safety regulations that would actually reduce employer costs and improve worker safety are blocked because of hubris, indifference and inertia, is SWA doing its job?
I thought I’d be a bit more forthright because expecting mining companies and government agencies to actually care about people exposed to lead is looking more and more like something that doesn’t happen.
Glencore is Australia’s biggest employer of lead risk workers, and since this whole thing started with them, keeping them in the spotlight seems quite reasonable to me. But don’t ever forget that there are a lot more industries involved that expose workers to lead risks.
I approached Glencore about 5 months ago to point out their (government-mandated) workplace health and safety procedures for managing lead biohazard safety of lead risk workers was harming their workers.
The safety procedures were formulated over 40 years ago when a lead exposure management policy was put in place in the US, which removed workers from lead exposure if their blood lead levels went over 60ug/dl. Once the worker’s blood lead level reduced below 40ug/dl, which was interpreted as indicating that absorbed lead had left the body, they were allowed to go back to work.
The only thing that has changed in that policy is that the blood lead levels have been halved to 30ug/dl and 20ug/dl respectively. That represents over 40 years of sloth, disinterest and disregard for the safety of lead workers on the part of occupational safety regulators. I had initially added ignorance to that list, but that’s not true because they know it’s wrong.
What’s wrong with this decades old policy is that a falling blood lead levelon removal from lead exposure does NOT mean any significant amount of lead has been lost, it just indicates that the lead has gone to other organs, and bone. If you’re reasonably healthy (no cancer) and an adult male, almost all the lead you absorb ends up in your bones (about 95%), where it stays and screws up your health for the next 30-40 years or so, if you live that long. The story for females is infinitely worse, but in a different way.
You could reasonably think that having found out that the existing workplace health and safety policy for lead risk workers was causing long-term harm to their workers, that Glencore would have welcomed suggestions on how to fix the problem. That’s certainly what I thought, but Swiss-owned multi-nationals have other priorities it seems, and avoiding long-term harm to their workers isn’t one of them. Denial and obfuscation, in whatever form, is how they handle things.
I pointed out that the potential for future legal action by lead workers who discovered their health had been screwed up by lead exposure. I suggested that Glencore HAD to know about the total body lead burden of workers to manage that risk. I’m talking about thousands of workers, potentially anyone who has done lead risk in Mt Isa for the last 40 years or so.
As long as it’s cheaper to handle worker law suits with out of court settlements and NDAs, denying there is a problem is probably reasonable from their viewpoint. In the absence of a working lead burden management policy, that almost makes sense in a truly disgusting way, since admitting there is a problem potentially opens a Pandora’s box of class actions by former workers. Then again, they had the defense that they were following regulatory mandates.
I think that it’s monumentally stupid and short-sighted view but who knows what goes on at head office. A corporate mentality that would rather spend resources on legal fees than even think of fixing a long-standing environmental health issue is completely at odds with their “public image” of a good community citizen.
I’ve pointed out that a woman of child-bearing age who has worked in lead risk work is carrying an awful legacy from the lead she has absorbed, because that lead will be passed to her unborn child through the placenta, and via her breast milk if she breast-feeds her child. That’s a case Glencore couldn’t win, about harm to a lead-affected mother and her lead-affected child.
I still have an issue with imagining how any company can miss seeing the potential for legal disaster in that scenario. Are their legal advisers so arrogant they can’t see that? Or does Glencore have some kind of “get out of jail” free card to avoid class actions? Then again, most of the lead risk workers are men, so maybe it’s no big deal.
But Glencore could defuse the legal liability of managing lead accumulation in lead risk workers by measuring accumulated bone lead and removing the lead. Surely, doing that would be much less expensive than endless litigation.
It would be a damn sight better for the workers too.
But since this is about trying to encourage Glencore to show a bit of sense, let’s look at what else is at stake. Lead affected adults suffer reduced cognitive ability, poorer decision making, and are more likely to be violent. They are more likely to die of poor decisions and more likely to die of cardiovascular disease, more likely to get cancer, renal disease and the list goes on. What does it say about a company’s basic culture if it ignores the consequences of it’s action, or in this the consequences of it’s inaction?
It is important to point out that inaction isn’t a crime within the scope of mandated lead worker safety procedures. I would not want to criticize Glencore for a failure to follow the rules, but following the rules blindly, without even an attempt to come up with something better, despite the fact that they now KNOW they are causing harm? That’s hardly praiseworthy.
And in that sense, the problem isn’t primarily with Glencore. It lies with the regulatory authorities (like Safe Work Australia) that have been too spineless to change something they know is wrong. This is not the way occupational health protection should work, and this appears to reflect failures at every level of government.
We have the technology and the knowledge to manage lead exposure risks as well as lead exposure. The problem is so neatly defined, the causes known, and the solution so neatly packaged that if we can’t eliminate this travesty of occupational safety, it’s because the government agencies are working actively to avoid doing anything.
We have the knowledge required to do something provided we have the political will. If common sense in our Health services translates to pressure on Safe Work Australia to update their ignorant and damaging policies, lead risk employers like Glencore will have to follow suit. This is only going to happen if it’s driven by community involvement and concern.
In the absence of any official interest in actively managing lead levels in the body, reducing exposure to lead is pretty much all we can do, unless we manage the problem ourselves, particularly for children. I’m going to make references to Mt Isa because that’s where this blog started. The comments apply everywhere in Australia where there is contamination from leaded petrol or lead paint.
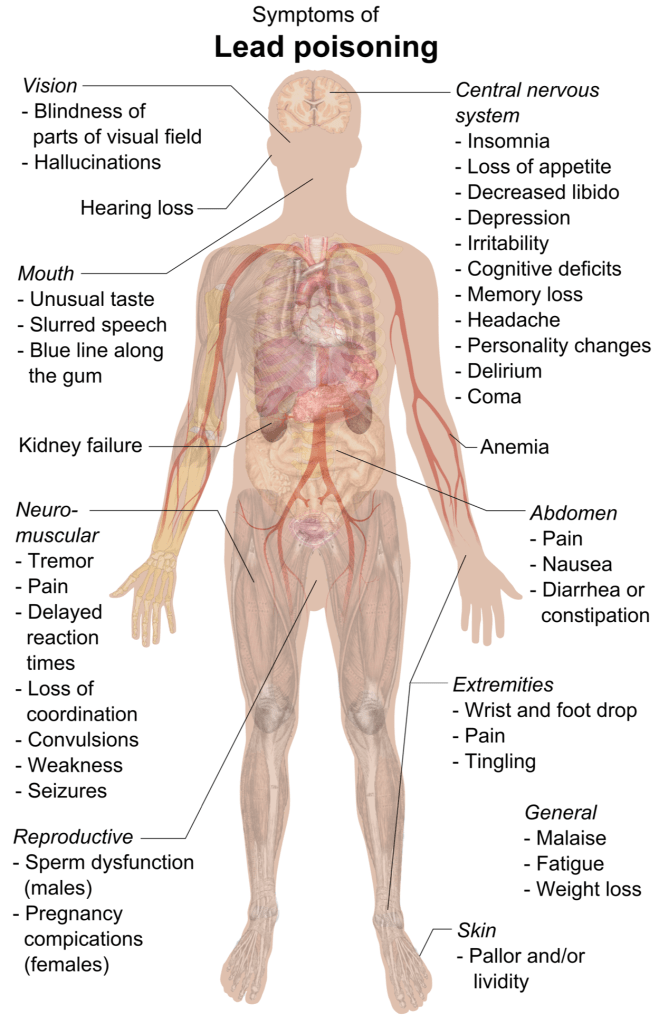
If you’ve been reading my blogs, you’ll realize that we need to appreciate that lead is so dangerous because it is a subtle poison that first affects the brain and nervous system, and then slowly damages other organs as body lead levels increase. Enough lead will kill you, but even low amounts of lead will cause some damage. There is no level of lead that is safe.
I’m going to repeat a lot of what I’ve already said in other posts because you really need to appreciate just what we’re facing.
My wife wrote a poem called “Terminal Man”. that I think is pretty amazing. I’d like to quote one paragraph, which is a terribly apt description of the mining industry:
Out in the countryside giant machines rip ore from the bowels of the earth, leaving it torn and bleeding. Factories belch clouds of ash and smoke into the atmosphere from taller and still taller chimneys, ensuring the acid a global distribution. Even in the most remote corners of the earth, trace amounts of toxic wastes are found.
I have to stop here and try and make the point that I understand the necessity of allowing mining from an economic viewpoint, It is pointless and somewhat self-defeating to try and shut down mining. BUT we have had nearly a century of lies and deceit about the dangers of lead, and one of the sources of those lies and deceit was the mining industry. In their defence, their efforts were minor compared to the paint manufacturers and companies selling leaded petrol, but they have some responsibility.
There is a Veritasium channel YouTube video about leaded petrol, entitled ” “The man who killed the most people in history” (https://www.youtube.com/watch?v=IV3dnLzthDA). It’s a really interesting story, and it makes the last part of the above poem excerpt terribly apt when it comes to lead and it’s dispersion around the world.
I’d like to continue with some historical and oddly current quotes that finish setting the scene:
From Benjamin Franklin (1786):
You will see … that the Opinion of this mischievous Effect from Lead is at least above Sixty Years old; and you will observe with concern how long a useful Truth may be known and exist, before it is generally receiv’d and practis’d on.
From Gordon Thayer (1913):
And shall we not signally fail of our guarantee of a reasonable surety for the health and happiness of all those within our borders, if this cry of suffering, now audible after many years of dumb endurance, remains unheeded and unanswered.
From environmentalist René Dubos (1969) who warned that the problem of childhood lead poisoning:
“is so well-defined, so neatly packaged, with both causes and cures known, that if we don’t eliminate this social crime, our society deserves all the disasters that have been forecast for it.”
These quotes and warnings span over 3 centuries, and remind us that change is a difficult process, particularly when there are forces working against change if they see that it benefits others at the expense of their profit. Workplace health and safety regulations have been essentially static for over 50 years except for a halving of the removal value from 60ug/dl. We’ve learned so much more about the harmful effects of lead on adults and particularly children that we no longer have the excuse of ignorance.
The US had the advantage of a society that for a time attempted to rectify socio-economic wrongs in America, epitomized by the disproportionate effects of lead on disadvantaged people. This spurred a huge effort to learn about and reduce the effects of lead, particularly on children.
While aboriginal and islander people are in a similar situation in Australia, we haven’t seen a similar rise of interest in understanding and minimizing the effects of lead on our indigenous people, or indeed the non-indigenous population.
I’ve come to the uncomfortable conclusion that we can’t depend on government agencies influenced by mining companies to do anything about reducing the risk of lead exposure in Australia.
It isn’t that there aren’t people in government that care, but government policies make sure that any changes pertaining to lead are very slow in happening, if at all. My opinion, on the basis of epidemiological information available, is that lead paint is a much greater risk to the population as a whole than asbestos. And yet we have only warnings, not legislated safe procedures for dealing with lead paint, unlike the US.
If you’ve been reading my previous (see below this one) blog posts, you’ve heard all the information about how lead harms you before. But please bear with me because you HAVE to realise that this information is about you and your family, and what lead can do to you.
What happens when you’re exposed to lead?
Once lead is absorbed from the intestine, it enters the blood plasma space. Red blood cells (RBC) have both a high affinity for and a capacity to hold lead. In a blood sample, about 97% of the lead is found in or on the RBC. Lead is transported in blood and delivered throughout the body.
Studies that used radioactive lead given to volunteers have shown that lead has a half-life in blood of a few weeks. In contrast, lead that accumulates in your brain has a half-life of 1-2 years and in bone, the tissue that accounts for up to 95% of the lead in an adult (about 75% in a child), lead will remain for decades.
Lead is distributed to all organs. Toxicity is mediated through several mechanisms. Calcium-binding proteins (eg, calmodulin, troponin) preferentially bind lead . Once lead has bound to those molecules, processes that are normally calcium mediated may be activated or inhibited, thus disrupting normal intracellular calcium-relayed messages. One of the mechanisms is calcium-dependent neurotransmitter release, resulting in altered intercellular communication. Enzymes may bind lead, resulting in adverse function. Lead binds to sulfhydryl and amide groups in enzymes, altering their configuration and diminishing their activities.
Lead interferes with heme pathway enzymes which are found in all cells. At least 3 of the 7 enzymes involved in the production of heme are downregulated by lead, resulting in a dose-dependent diminished production of heme and in the accumulation of precursor molecules. The appearance of precursors like protoporphyrin were used before BLL to indicate lead exposure.
I nearly forgot to add that lead also causes extensive free radical damage to organs, cells, cell membranes and DNA, contributing to conditions like atherosclerosis and Alzheimer’s.
As lead substitutes for calcium in the skeleton, it results is weaker bones and slower fracture healing, but most importantly, lead in bone acts as a reservoir of lead that maintains circulating (blood) lead levels.
As the amount of lead in our bodies increases, so does the functional interference and damage to organs, and the brain is the organ most affected by even low levels of lead.
I hope that’s plain enough, even small amounts of lead do some harm and as the amount of lead you’ve absorbed increases, so does the harm.
It’s a great pity that the only tool we’ve got for “measuring” lead exposure at the moment is blood lead levels (BLL) There are other options possible to measure body lead, but they aren’t generally used in Austrlia, at least not for humans. So BLL is pretty much the only tool in our toolbox. A bit like the story about the carpenter who only had a hammer, so everything looked like a nail. A lot of decisions about safety and treatment are made that rely totally on BLL.
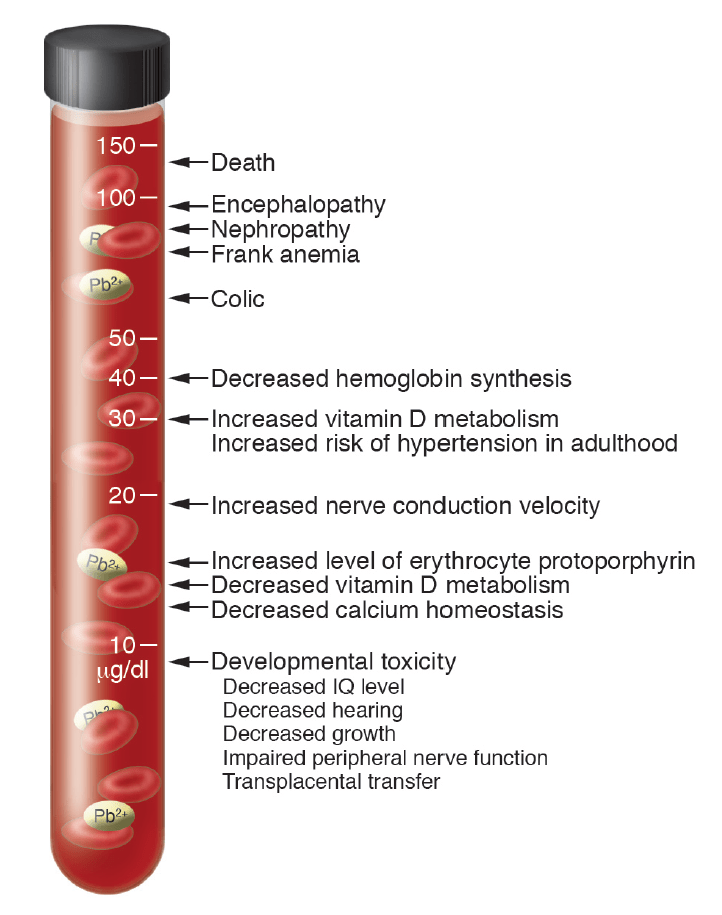
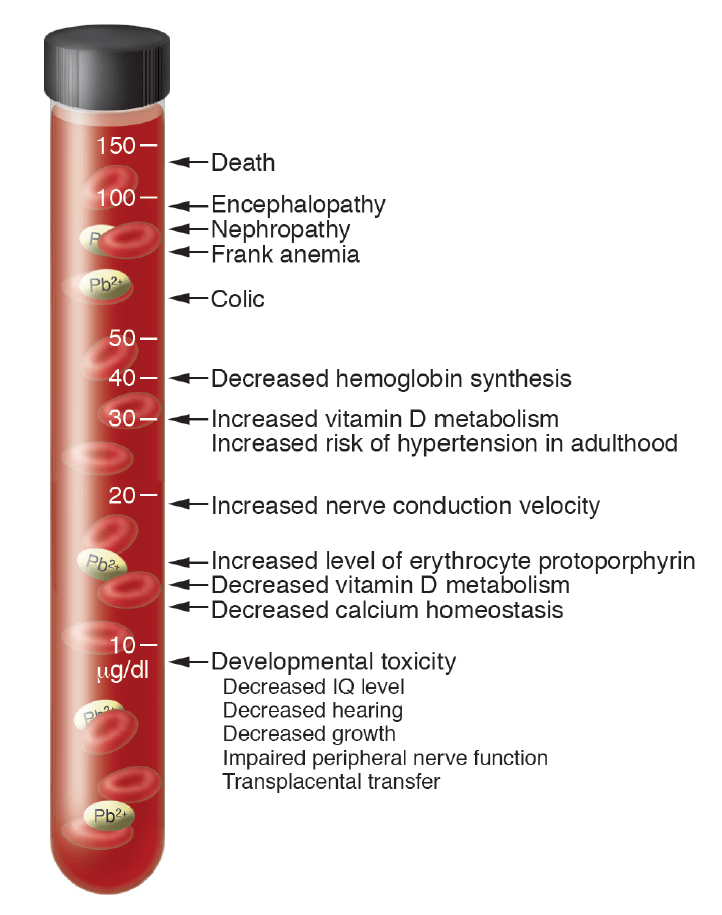
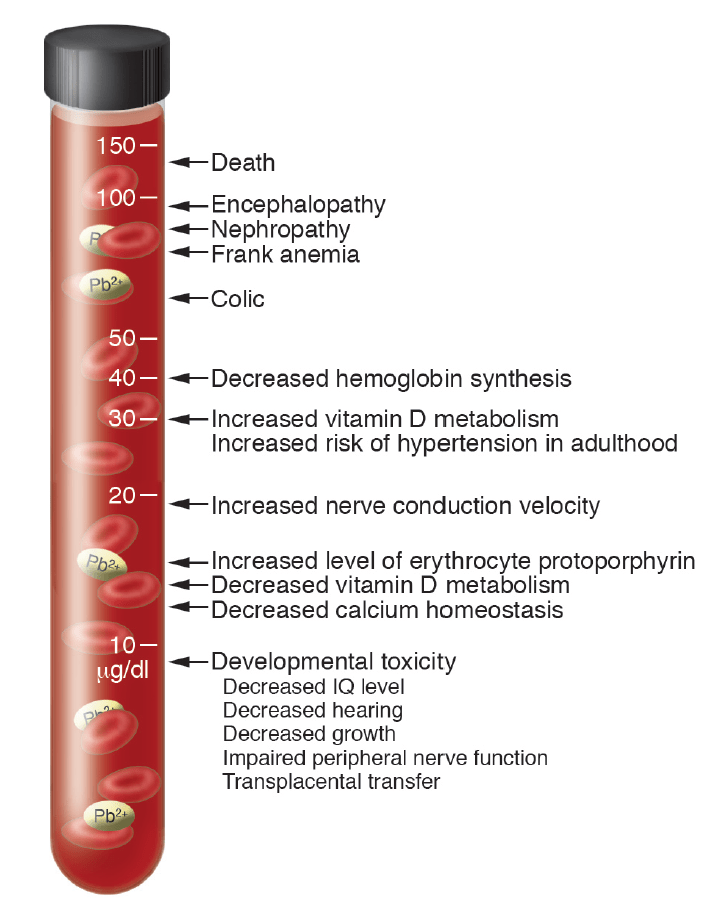
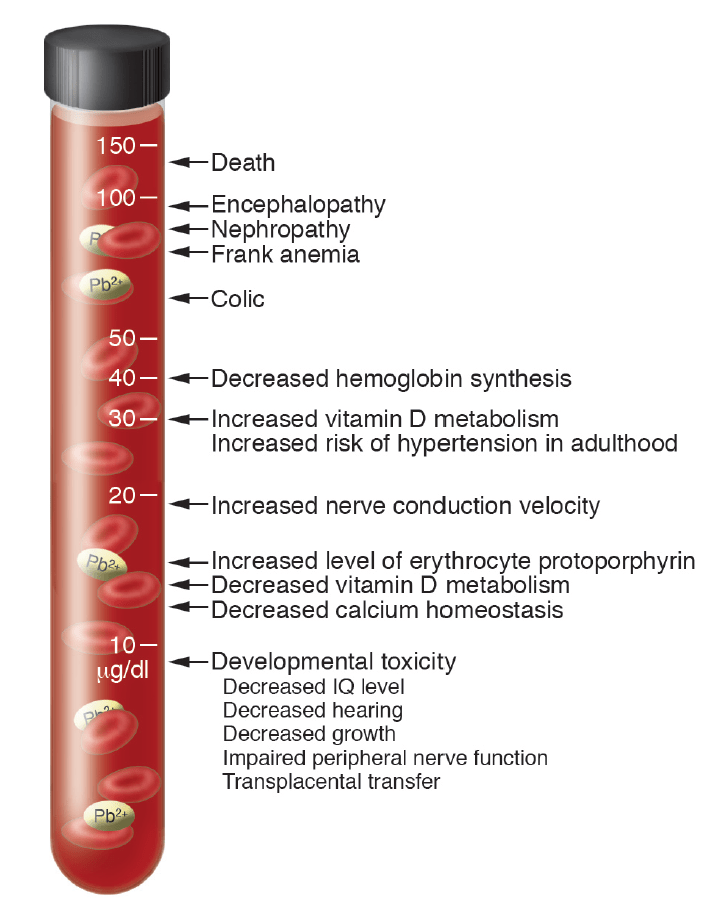
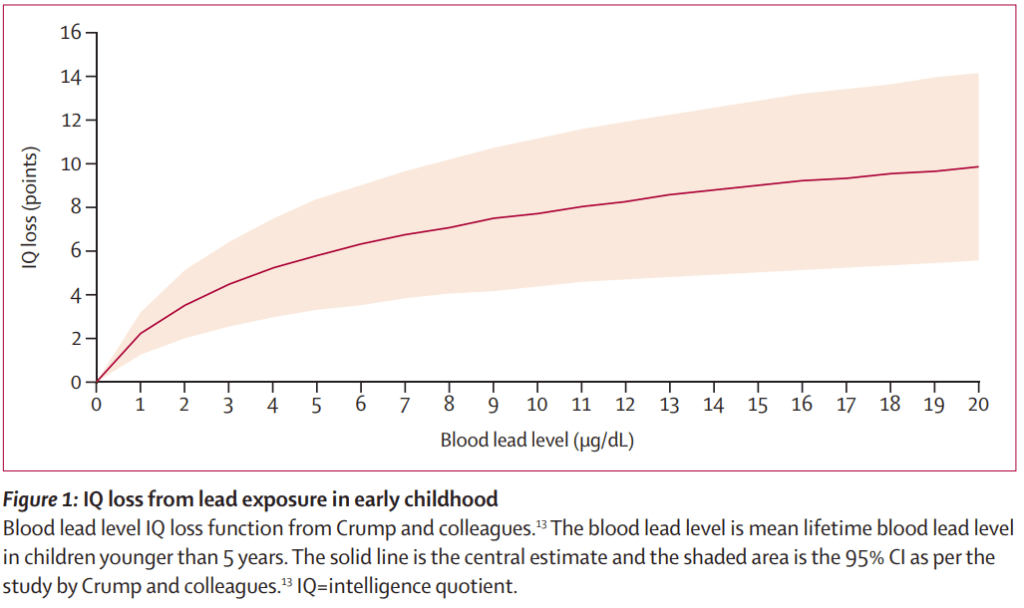
I’d like to provide a bit of extra emphasis about what lead does in your body, so let’s use my favourite chart again:
This is what you will see as BLL rises: (this leaves out the 7-fold increase in esophageal cancer at 30ug/dl and the doubling in cardiovascular deaths at 10ug/dl)
There is a huge problem with our reliance on BLL because it is solely a measure of how much lead is circulating in the blood not how much lead is elsewhere in the body. BLL only measures lead in one of the body’s pools of lead, the blood.
If you go back to my description of what happens when you absorb lead, some of the lead binds to red blood cells (RBC), the rest goes to other organs, the brain and the bones. BLL indicates the sum of the lead that is bound to red blood cells, and the lead contribution from lead already stored in your body.
After exposure, as the red blood cells containing lead get broken down over a period of several weeks, your BLL will fall because the red blood cells that bound lead are being broken down.
The single biggest misconception about BLL is that a fall in BLL after exposure means you’ve lost the lead you absorbed. A little bit of lead is lost but most of it stays and as I’ve said, it stays there for decades, often the rest of your life. As you absorb lead from food, or from renovating a house, shooting a gun or rifle, repairing electronics and so on, you will slowly accumulate ever more lead.
I do have to qualify that statement because there are times when lead can be rapidly released from the bones: pregnancy, breast-feeding, osteoporosis and some blood cancers. though I doubt that provides some comfort to mothers that they can get rid of the harmful lead in their bodies.
The rise of BLL after exposure to lead and the fall in BLL in the absence of lead exposure is used to “manage” lead exposure in lead risk workers.
This is where I started with Glencore and what I viewed as insane lead biohazard management.
Lead risk workers get their BLL measured regularly. If you’re a lead risk worker and you’ve either been careless, or there is more lead pollution in your workplace that you couldn’t avoid, you’ll absorb extra lead. As a result, that lead will get into your bloodstream and your BLL will increase. If your BLL goes above 30ug/dl you get removed from lead risk work.
While you’re away from exposure to more lead, your body is breaking down red blood cells that have bound lead which appears in your bile, but most of the lead absorbed is moved to your bones. That decreases the amount of lead in your blood, so the BLL will decrease. When your BLL goes back down to below 20ug/dl, it’s deemed okay for you to go back to work, presumably in the belief that the lead you’ve absorbed has left your body.
That was certainly the belief over 50 years ago, despite the fact that even then it was recognized that most of the lead absorbed went into bone. If you take tissue samples, including bone during autopsy, most of the lead is found in the bones.
The Glencore principal health and hygiene made the following comment in a letter to me:
We have a range of stakeholders, including health experts that we engage with around the management of occupational exposure, with the implementation and monitoring of any measures based on strong clinical evidence and supported by peak medical bodies and State and Federal Government.
And the health experts missed the strong clinical evidence that lead bioaccumulates in bones? If we assume that the experts do know better, the only other explanation I can think of for not updating the ”management” of lead exposure, namely monitoring and removal, is that everyone involved in the occupational health area thinks it’s more important to manage excess lead exposure, than to manage lead risk worker health.
I admit that if the lead HAD left your body, removal would make sense, but that’s not what happens. It achieves nothing, except giving the worker and employer a false sense of security. Employers, if they know the truth, which is certainly true for Glencore, since I’ve told them, are looking the other way while their workers continue to accumulate a deadly legacy.
It’s not about worker safety or worker health, it’s all about exposure control.
I absolutely get the idea of managing lead exposure, because that manages an important part of the total risk of accumulating lead. But surely there has to be a better way than using lead risk workers as ultimately disposable lead exposure detectors, like mine canaries in a coal mine?
The challenge with biohazards is they’re invisible, not like a crushed foot or a death in the mine. Aside from the dust from the mine, or the fumes from the smokestack, they’re invisible. We can manage obvious hazards, but biohazards are a bit like magic, so sometimes managing them uses sleight of hand. Workers “think” they’re being kept safe, but that’s not really the case at all.
We have to do better, we could do better IF a few people woke up to the harm being done to workers. SWA know from a Monash study that as BLL increases, so does the incidence of cancer, so does kidney disease, so do cardiovascular deaths and so does neurological disease and behavior changes. They admit they know this on their web site. But the regulations haven’t changed.
I hope I’ve explained what BLL means and what lead does, so let’s get stuck into non-occupational lead exposure reduction, because that is what this whole thing is about. After all, occupations that are exposed to lead are well protected and managed. Damn, that sounds like sarcasm.
Reducing exposure to lead is the only option we “appear” to have at the moment for limiting some of the effects of lead on our health. I’d like to add that bone lead levels can be easily measured without any needles poked into you, but not in Australia. We can measure bone lead levels in wildlife, but it’s too hard to do that for humans, or maybe it’s because it would expose the awful truth of generations of poisoned lead workers.
I’m pretty sure I wrote a blog on the sources of lead exposure but I’m going to concentrate on the big ones, lead from buildings painted with lead paint and lead in the environment (natural, mining/smelters or leaded petrol pollution). .There’s also lead from old lead acid batteries, lead paint on motor vehicles and boats and lead from using firearms, and a host of minor sources of lead, but let’s put the effort where it counts.
Just about every single house in Australia that was built before 1975 will likely have been painted with lead paint. If you’re in Brisbane, for example, that means thousands of housing commission houses on the outskirts of the city (50 years ago), not to mention older stately homes.
Lead paint has been a huge danger for children and animals because it tastes sweet and is nearly irresistible to children and animals. Children have died from licking lead paint. Queensland clinicians have recognized lead paint as a grave danger to children since the early 1900s but they now seem to have forgotten the early lessons.
And the lead paint is still there, today, right now. Every time a house or building painted with lead paint is sanded or renovated, paint dust, containing up to 50% lead, kilograms of it, is spread around the house, in the yard, in neighboring yards. That’s pretty major lead pollution. Would it surprise you to learn that painters are high on the list of lead affected individuals? It’s a pity we don’t know how many children are affected,
In the United States, lead paint is recognized as gravely dangerous for children, and the EPA legislation “Renovation, Repair and Painting” (RRP) has been enacted to minimise the risk from renovating old buildings:
Under the rule, contractors performing renovation, repair and painting projects that disturb lead-based coatings (including lead paint, shellac or varnish) in child-occupied facilities built before 1978 must be certified and must follow specific work practices to prevent lead contamination. EPA’s RRP rule impacts many construction trades, including general contractors and special trade contractors, painters, plumbers, carpenters, glaziers, wood floor refinishers and electricians.
Activities performed by all of these trades can disturb lead-based paint and have the potential to create hazardous lead dust. For most individuals, eight hours of training is required. However, individuals who have successfully completed renovation courses developed by HUD or EPA, or an abatement worker or supervisor course accredited by EPA or an authorized State or Tribal program, can become certified renovators by taking a four-hour EPA-accredited renovator refresher training.
That looks a lot like the regulations about asbestos in Australia, because asbestos was finally recognized as dangerous, probably because it’s no longer mined in Australia. While the various Australian EPA and health organizations do have warnings about the dangers of renovating lead-painted buildings, there is no protective legislation, only an Australian Standard.
A quote in a 2018 RFI document from a senior Queensland Health employee in Townsville makes an interesting point about lead paint:
“As things stand, I do not believe that government owned houses, with highly contaminated soils andexposed Lead paint, are safe places for children in Mount Isa. Rehabilitation of known contaminated environments is where we need to act,“
So what are government agencies doing about lead exposure from renovating old buildings? Pretty much nothing.
That kind of makes protecting you and yours from lead paint a bit more difficult doesn’t it?
I guess it’d be okay if getting a blood test for lead exposure was common and you could remove any lead that was absorbed, but avoiding exposure to lead paint is something where there’s very little good advice that I can give you. Sorry.
The only real solution is what the US EPA did, and I can’t see that happening here. It is my sad belief the mining companies have a firm grip on the decision of parts of our governments agencies.
Lead dust exposure is the other big one, though I’d like to exclude lead dust from leaded petrol because that’s a big city problem. I’d like to concentrate on the lead dust affecting the people living in one of the lead cities, or that live near the Port of Townsville when the wind is blowing their way when ships are being loaded with lead concentrate.
It is ridiculous to think, in Mt Isa, after 90+ years, that the lead contaminated yards, the lead-containing dust in the houses, in the attics, is all due to natural causes. Who do they think they’re kidding? The real tragedy is some people in Mt Isa are certain that lead isn’t a danger.
Lead dust, from crushed lead-containing ore or lead concentrate, or from smelting lead ore gets into everything. It settles on the ground, on roofs, it washes into rainwater tanks. Plants or animals grown on lead-contaminated ground absorb the lead. If you’re scrupulously careful and make sure children don’t play in the dirt and don’t touch anything covered in lead dust without washing your hands afterwards, you’ll get by. One badly contaminated yard in Mt Isa was “fixed” by removing the grass and trees, covering the yard with concrete and adding artificial turf.
While that’s a wonderfully creative way to stop kids playing in contaminated dirt, I can’t help wondering if that’s the best possible solution.
In the absence of due diligence and monitoring by an agency other than the polluter, community monitoring is probably the only thing that will work. That should be the role of the EPA, but often isn’t because there is always a political component. A when a previous EPA director gives evidence on the behalf of a miner, you have to wonder about influence.
There is a “solution” to this problem, and that’s to use a compound possibly used at the smelter to remove heavy metals from the flue gases. Glencore very likely have some. It makes lead biologically inert and works brilliantly to decontaminate heavy-metal contaminated sewage and soil.
If you rely on rainwater, then you’d better filter your water before you use it and get an air purifier for you house because it will mop up a lot of the dust in the air. A vacuum cleaner with a HEPA filter would be useful too.
I have a blog post on how to protect yourself and your loved ones from lead exposure, but lead paint is a challenge.
Let’s talk about what the health services do in the event of excess lead exposure.
The medical term for doing things to reduce exposure to lead is intervention. If a child has raised BLL, medical authorities will instigate an intervention to reduce lead exposure. I’ll describe the process below.
It’s hard to get the intervention order below quite right, because in the past, the job of detecting the source of lead exposure came after signs of exposure. However, depending on the tools used, detection can happen first. So the approaches to reducing exposure are:
(1) Detection, know your enemy. You need to know where the lead is so you know where to focus your efforts. In the past that meant sending samples off to be tested or using insensitive lead test kits, but the possibility now exists to quickly measure lead contamination with a portable x-ray fluorescence spectrometer (XRF). One very interesting sentinel for high environmental lead levels is your dog or your chickens if you have some (just don’t eat the eggs). High BLL in dogs or chickens means high levels of exposure around your house. Ask your vet.
(2) Reduction of lead contamination. Anything you can do to reduce lead exposure is a step in the right direction. That can be really difficult if you’re living in a pre-1970s house that is covered with lead paint. While there are EPA guidelines which stress being careful about contamination when renovating an older house, anyone can sand a house without taking any care to minimise the spread of lead paint chips ad dust. I’ve written a blog (just scroll down) on some of the things you can do.
Then we get to something that is eminently possible, something that has been in use for over 60 years, and something that isn’t used unless clinical signs of lead poisoning are present, removing the lead.
(3) Where lead exposure can’t be prevented completely, removal of excess lead. That introduces the concept of chelation which is regarded as quack medicine by most of the medical industry, for no currently justifiable reasons. Why is chelation a normal treatment option in places like Italy, and not used except in extreme need in Australia (and the US and UK)? It’s a long story I’ve covered in other blog posts.
I’d like to provide more information on intervention (doing something to reduce lead exposure) to reduce lead exposure and what triggers intervention.
In the United States it is quite common to test for blood lead levels in children and in adults, even those not in lead risk occupations. Unfortunately, that isn’t the case in Australia, with the exception of occupational lead risk workers and children in Port Pirie, Broken Hill and Mt Isa. There is very little testing otherwise so while the detection of children with raised blood lead levels is not at all uncommon in the US, and again with the exception of the lead towns of Port Pirie, Broken Hill, and Mt Isa, testing for lead is relatively uncommon in Australia. The situation with non-occupational testing of adults is no better.
If a child’s blood lead level (BLL) is above the notifiable level, now 5ug/dl, a number of interventions are undertaken. If the BLL is above 45ug/dl, lead removal by chelation therapy is a recommended option.
There are differences in the extent of intervention.
In the US intervention consists of
Education for caregivers (which includes nutritional advice and information about reducing exposure in the home); a voluntary home environment investigation; and a referral to lead remediation services. A more intensive intervention can be triggered by tests over 15ug/dL or 20ug/dL. In addition to educating caregivers and providing a referral to remediation services, the intensive intervention typically includes: a mandatory home environment investigation; nutritional assessment; medical evaluation; developmental assessment; and a referral to the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC).
There are also subsidies available for lead-painted wooden window replacement in older houses, lead paint remediation services and replacement of lead plumbing.
Intervention in Queensland is similar: investigation, restriction and counselling. The intervention isn’t as thorough or complex and the other stuff like subsidies for rectification work to reduce lead exposure, and nutrition advice on reducing the effects of lead don’t exist.
There is no treatment for sub-clinical lead poisoning.
This is a basic flaw in intervention and lead exposure reduction insofar as it mostly doesn’t do anything if the child has been exposed to lead for long enough to accumulate significant bone lead stores.
My opinion is that raised BLL is something that should be treated in the same way as snake venom or infections, or diabetes because if no treatment is applied to remove the lead, something will go wrong.
I’d like to provide a some encouragement as to the importance of reducing lead exposure. I mentioned that due car and hygiene (and nutrition) will limit the amount of lead absorbed. If body lead levels can be kept low enough, particularly between the ages of 0-4 years, some serious neurological effects can be avoided. That means avoiding or minimising behavioural problems and educational problems, and that’s absolutely worth doing.
Why would we not want to give our children as good a chance at a normal life as possible. How can we possibly think of our children as disposable because it’s too hard to manage the problem of lead exposure?
That is probably a good place to emphasize another important difference between the US and Australia. In the US intervention and rectification is a multi-agency activity, because the effects of lead on children includes cognitive decline and behavioral problems, which have a direct impact on education and the youth justice system and well as health issues. Dealing with the problems of health exposure aren’t just the responsibility of the health authorities or considered a “pollution” issue for the EPA.
In the absence of a whole of government initiative, we won’t see any real progress in minimizing lead exposure.
How can Queensland Health effectively protect children if other government departments don’t get involved in fixing their part of the problem? This is a issue not just for Health, but also Education, Youth Justice, Public and Community Housing and the EPA. That’s a challenge because unless the Premier’s department gets involved, what is the likelihood of multiple ministries working together?
Another challenge is community attitudes.
As an example, the biggest advances in reducing lead exposure, and children’s lead levels happened in Broken Hill when the local community got actively involved in exposure reduction for children.
Would it surprise you to find that approach is much more useful in reducing childhood lead exposure than denial?
Ignoring the problem, insisting there’s anything wrong, or even harassing people that speak up about protecting their children being as important as protecting their jobs, does not fix the problem. A community working together, recognizing the challenge and dealing with it can deal with the dangers of lead. That’s without risking jobs or property values, or stirring up prejudices. Mt Isa does not have to accept that children getting poisoned is part of the cost of living and working in Mt Isa.
You’ need to know that a portable x-ray fluorescence spectrometer (XRF) could be used by the community to detect lead contamination in your houses and yards.
Empowering the community with the means to detect and resolve lead pollution is by far the most powerful way to protect your children. Broken Hill hasn’t shut down so why would getting Glencore to clean up their act a bit more, and community action for the real good of your children harm Mt Isa?
The sad answer is absolutely not, but we have no way of knowing because of the apparent lack of action by so many government agencies.
It is entirely possible, that like the US, Australia is lead poisoned. If we look at the history of lead in Australia, the lack of governmental action with regard to lead exposure in the general population, and the failures in occupational lead safety, this is not an unreasonable conclusion. With less than 1 in 2000 Australians tested for blood lead levels, there is also no credible data to dispute this claim.
There is also evidence of active suppression of information and alteration of safety decisions about lead, and little sign of any proactive action to either recognize or minimise the effects of lead on the population of Australia.
The story of lead in Australia has clear parallels with the much better-known story of asbestos. Just as with asbestos, public authorities were faced with a difficult choice between economic prosperity for the mining industry and safeguarding the health of workers and the public. We know how well that turned out, denial there was a problem until that didn’t work anymore.
I want to add a bit of historical perspective to the comment about active suppression:
Dr Leslie Jon Jarvis Nye was a physician in Brisbane. His 1933 paper in the Australian Medical Journal, “Chronic Nephritis and Lead Poisoning” so concerned the Lead Industry Cartel that they commissioned a “scientific” monograph to refute it.
Although anti-lead paint legislation had been enacted years previously, it was being ignored. With support from the Premier, Forgan-Smith, and the Communist secretary of the Painters’ Union, Dr Nye was able to explain to a meeting of painters the dangers associated with lead paint and from then on, they refused to use it.
I suspect whatever has replaced the lead industry cartel is still unfortunately alive and well. And anyone trying to make the public aware of the dangers of lead might have problems.
If you were living in Australia between 1930 and 2000 you would also have been exposed to the lead from leaded petrol, and that lead continues to contaminate areas near major highways even today. Light aircraft still use leaded petrol so don’t live downwind from a general aviation airport.
Lead paint has been a curse that was recognized since the early 1900s and while high levels of lead were “technically” banned as early as 1922 in Queensland, it continued to be used for another 40years or so. Industrial paints weren’t included in the lead ban in house paints so automotive paint is still available with up to 20% lead.
I would like to quote a 1955 investigation, which found:
“Victorian houses in Queensland characteristically had closed verandas, painted with lead-based paint. Such verandas were ideal for confining small children while their mothers were busy in the house. From daily rain showers in this subtropical region, rain droplets hung on the railings and tasted sweet from dissolved lead. They were within the reach of toddlers, who enjoyed wiping up and licking the rain droplets.”
Renovating pre-1970 houses (some a bit later) painted with lead paint is a huge hazard for the painters, the occupants and any children in the vicinity.
So while the problem of inhaled lead from leaded petrol is now history, the legacy of leaded petrol still remains in the dust in attics, in the soil and anywhere near renovated older houses.
The level of non-occupational lead testing is so low that we have no idea of the magnitude of the problem. I have quoted the 1999 figure of less than 1 in 2000, and can now update this with figures from Medicare (2014) which indicate the testing ratio is no higher. The NHMRC recommended against wide-spread blood lead testing in their 2015 report so the testing ratio is now probably lower. How things have changed.
I would love to be able to state something useful about the degree of risk to the community, especially to our children of historical sources of lead poisoning, but I can’t. Nor can ANY government agency assure us that the dangers of lead are reducing, because without more testing we just don’t know.
But let’s get back on track.
Before I go on, I’d like to point out that there’s a blog post of mine a couple of blogs down from this one that gives hints on how to minimize lead exposure.
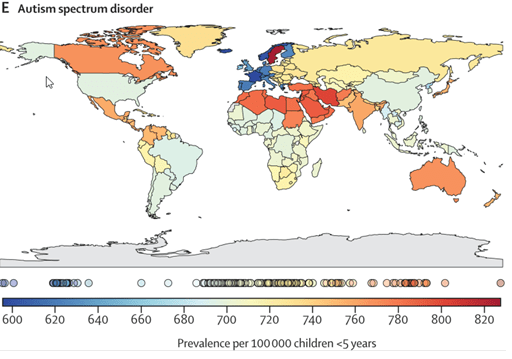
Since infants are the most affected by lead exposure, that might be a good place to start in asking a few questions. Here are a couple of incidence maps for autism and ADHD.
The rate of autism in Australia is about the same as Canada, and a bit more than India. Since this blog post is about lead, I can’t help pointing out that if a baby is exposed to a significant amount of lead, he or she can exhibit autism-like symptoms, and if you’ve read Nancy Hallaway’s e-book you’ll also have realised that at least some of the neurological symptoms can be resolved if the lead is removed.
Considering the opportunities there are for lead exposure in Australia, it would be fair to speculate that at least some of the cases of autism may be caused or contributed to by lead exposure. Something as simple as renovating an old house, sanding off the flaking paint while there are infants nearby, can result in lead poisoning and the symptoms of autism. Living in a lead-rich environment is another scenario where an infant could end up with sub-clinical levels of lead. I use the word sub-clinical because the “clinical” symptoms of lead poisoning are considered to be the ones we’ve known for more than the last century. Oh how this needs to be updated.
There are undoubtedly other causes of autism including genetics BUT one of the possible causes is lead exposure. Why would we not want to filter out those kids and maybe even treat them to reduce the severity of the symptoms? You know, the kids in the older suburb where a lot of houses are being renovated as older people move to retirement villages and younger families have moved in?
Even if the incidence of lead-induced autism was 5%, as an example, that means that 1 in 20 kids with autism could potentially be able to develop normally if they were diagnosed with lead poisoning and treated.
That of course raises two issues, the first that with the exception of children in the lead cities, Broken Hill, Port Pirie and Mt Isa, there is next to no paediatric testing of blood lead levels. And even if the blood lead levels are well above the notifiable limit, the only clinical treatment children will get is chelation therapy IF the blood lead level is above 45ug/dl. Children with non-toxic blood lead levels (less than 45ug/dl) are not treated to remove lead.
That’s a big deal when you think about it. Children with levels of lead known to have harmful neurological effects, do not have the lead removed because they have “sub-clinical” levels of blood lead.
That’s kind of depressing because it’s almost like there is no recognition that lead accumulates in the body. Lead poisoning is subtle, it can be the result of a brief and intense exposure which produces severe clinical symptoms, or something can happen after months and years of lower-level exposure when you’ve accumulated enough lead to produce chronic symptoms or damage to internal organs.
One of the additional challenges to getting treatment for children with sub-clinical levels of blood lead is a widespread belief in clinicians in Australia that chelation is high risk, that it isn’t effective, or that it’s more important to reduce exposure as much as possible.
I know I’ve done this to death already, but it is so WRONG that I need to keep hammering at these misconceptions until people realise that chelation should at least be tried.
The early use of chelation, more than 70 years ago, sometimes resulted in renal failure and death. By the 1960s it was known that the renal failure and subsequent deaths were due to trying to do things too quickly, too high a dose, too often. In fact, it has been found that at much lower doses, EDTA could actually reverse existing renal damage because it acts like an anti-oxidant. IV chelation with EDTA that follows now established protocols does not lead to renal damage or death provided those, safe protocols are followed.
A 5-year old autistic boy died of hypocalcemia during IV chelation therapy. I can’t argue that chelation didn’t kill him, but when I looked up the case, which I thought was due to medical ignorance it turns the pharmacy supplying the EDTA for his chelation therapy prepared a solution of Na EDTA instead of the Ca Na EDTA that had been requested by his paediatrician. Na EDTA is used to treat hypercalcemia because it removes calcium from the blood. Ca Na EDTA is normally used to remove heavy metals like lead because it DOESN’T remove calcium from the body. The child died of hypocalcemia, which caused heart failure. That is an absolute tragedy, a child dying because they were given the wrong drug, the wrong form of EDTA.
But another tragedy has been the many children that maybe could have been helped, that weren’t because of the wide held “belief” that a child can die from chelation therapy because of this incident.
Ca Na EDTA does bind other heavy metals besides lead, like arsenic, cadmium and mercury. As I’ve said before, that’s a bonus, but it also binds zinc and magnesium, which are essential metals. One of the important adjuncts to chelation therapy is trace metal supplementation.
It’s worth mentioning that another use for Na EDTA, beside treating hypercalcemia, is to remove calcium plaques (atherosclerosis). It works quite effectively, though it has to be accompanied post-treatment with trace metals plus calcium. A sad example of chelation therapy being badly understood is that the California Medical board banned the use of Ca Na EDT because it was ineffective at treating atherosclerosis (removing calcium).
Administered with appropriate protocols and caution, IV chelation therapy has been proven to be safe. If it was so dangerous, why do they use IV chelation therapy on children with severe (over 45ug/dl and encephalopathy) lead poisoning? And use an oral chelator if encephalopathy isn’t apparent.
Another argument against chelation therapy is that it isn’t effective because blood lead levels “rebound” after chelation.
When lead is absorbed, most of it ends up in the bones. This varies from about 75% in children to 95% in adults. The lead in bones is in balance with lead in the blood and soft tissues. When a chelator is administered, it binds the easily accessible lead in the blood and soft tissues. If the chelation therapy doesn’t go on for long enough (most treatments are for 5 days) then very little bone lead is removed. Once chelation stops, a new balance between bone lead and blood/soft tissue lead is established, and blood lead levels go back up to a level that reflects bone and body lead levels. A rebound simply means you didn’t remove all the bone lead, not that chelation doesn’t work.
I’d like to quote the first sentence of the acknowledgemnt in the book “Brush with Death” by Chritian Warren:
Writing acknowledgements is similar to receiving treatment for lead absorption: a single course of therapy is supposed to abate a burden that had accumulated over many years. The patient feels better, some of the burden is lifted, but the bulk remains forever bound up in the bone.
Removing bone lead is a case of slow and steady lead removal, with a dose of chelator that is low enough to be absolutely safe, over many months until ALL the lead is gone.
I’m not going to argue that reducing exposure isn’t critically important, because it is. Successful campaigns to reduce lead exposure, for example in Broken Hill, have absolutely resulted in a lower mean blood lead level in children. It would be wonderful if exposure could be reduced to zero, but that’s pretty unlikely. The basic problem with relying solely on the prevention of lead exposure is that there are so many possible sources of lead, that it will at best only ever be a partial solution. Whatever lead is absorbed, will increase the body lead burden, and increase the risk of disease.
The lead that has been absorbed, that is stored in bone, is going to be there, and will keep increasing, unless we can do something about removing it. Diet can play a significant role is reducing absorption of lead, some food ingredients like citric acid are weak chelators, so in the absence of lead exposure, an appropriate diet could gradually reduce body lead levels. But if you want to remove lead in something less than decades, using a chelator that is reasonably specific for lead is a pretty good move.
I’ve talked about this before, but I think this is the right place to bring it up again. Cattle in far North Queensland graze on land that has naturally occurring lead deposits (not due to pollution from mining/smelting) and they have high enough lead levels that they have (recently) been found to be unfit for consumption. Some smarter than average station owners use a chelation agent which is used to remove heavy metals from flue gases, TMT 15, to remove lead from the cattle, and make them fit for consumption. TMT has such a high affinity for lead that it can remove all the lead from the cattle in a few weeks. I wouldn’t use TMT 15 on humans because it hasn’t been tested on humans as far as I know, but if we can remove lead from the cattle we eat, why can’t we remove lead from our children, and ourselves.
Whilst Australia continues to be a world leader in lead mining, smelting, and processing, the adverse impacts associated with production have been consistently downplayed by industry, governments, councils, health officials, and regulators. Even some academics argue the effects of low lead exposures are not of significant concern. Due to ignorance, misinformation, and deliberate obfuscation of evidence, generations of families living next to lead-mining, smelting, and refining centres such as those in Broken Hill, Port Pirie, and Mount Isa, have been and continue to be exposed to environmental lead, a known neuro-toxic contaminant.
More than a century of IQ-lowering poisoning continues
Childhood exposure to lead has been linked to lower IQ and academic achievement, and to a range of socio-behavioural problems such as attention deficit hyperactivity disorder (ADHD), learning difficulties, oppositional/conduct disorders, and delinquency. The disabling mental health issues from lead exposure often persist into adolescence and adulthood.
There’s a lot more and I would encourage you to read the whole article. While Mt Isa has only had a lead smelter for a bit over 90 years, it is unlikely that there has been any less lead pollution, except perhaps in the last 15-20 years.
I guess the point I’ve drawn from the Port Pirie example is pretty obvious in the title in the Conversation article, ”a long history of looking the other way“. That’s what Queensland Health (QH) have been doing for at least the last decade, possibly longer. I don’t mean the whole organization because I know there are people in QH that are deeply concerned about lead in children, but apparently not the bureaucrats.
I am pleased to have found out there is serendipitous testing of blood lead levels in children in Mt Isa. When blood sample are taken from children in the Mt Isa hospital, any excess blood in the sample is tested for lead. If high (greater than 45ug/dl) levels of blood lead are detected in children , they are treated to remove excess lead. Lower levels of blood lead result in activities to minimise lead exposure, but no treatment to remove lead. This is despite a huge amount of clinical and epidemiological data that blood lead levels as low as 5-10 ug/dl can have serious neurological consequences.
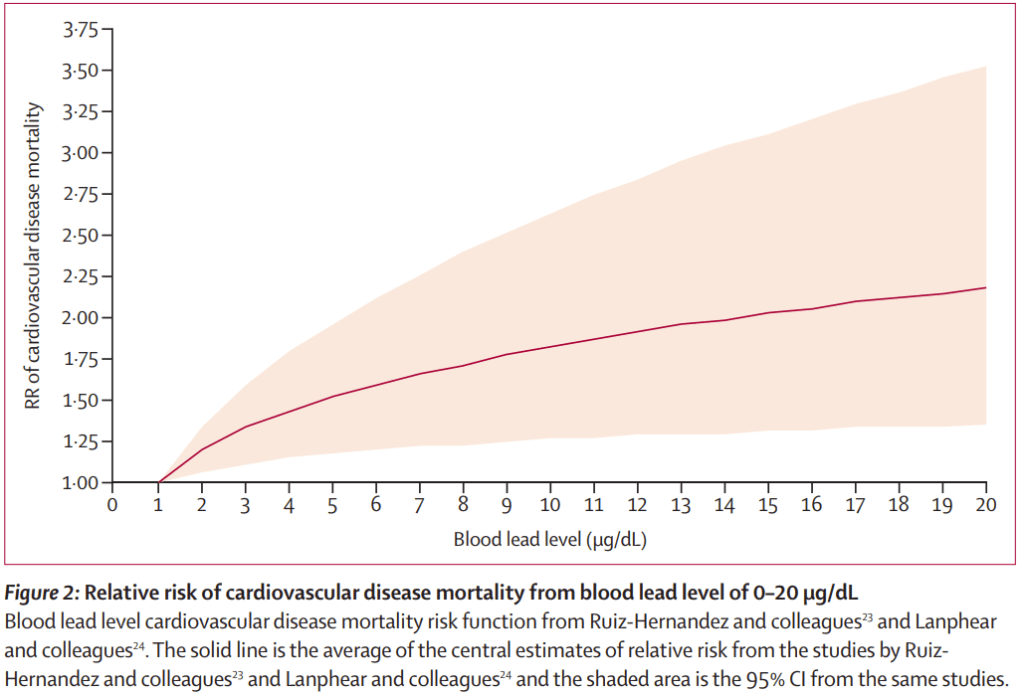
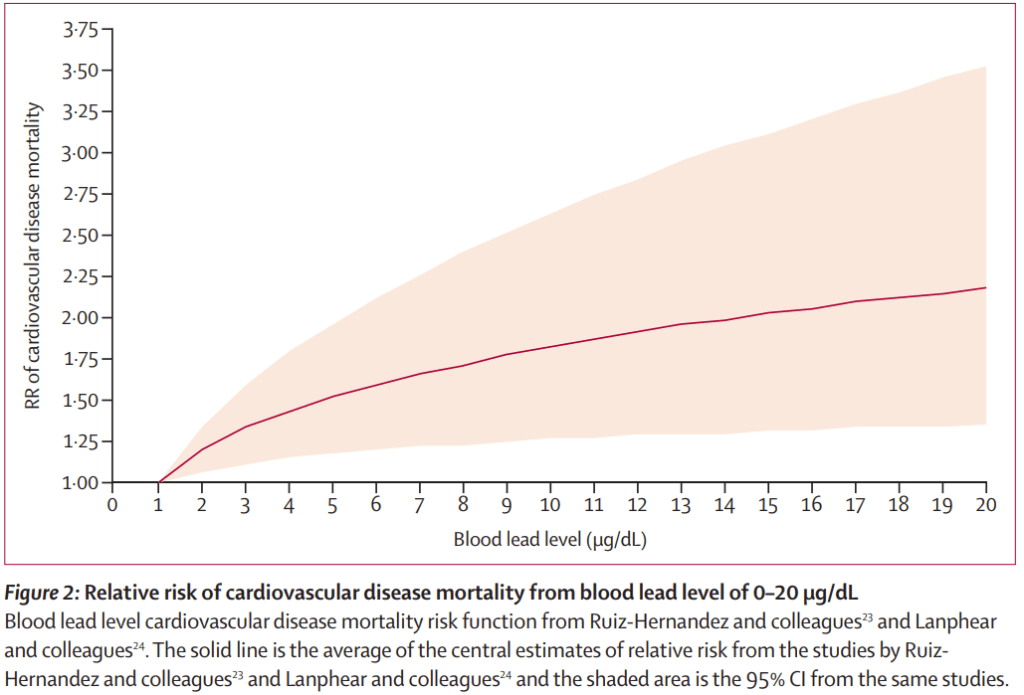
There is voluntary testing available for adults in Mt Isa (and children, though infrequently). In adults, anything under 75ug/dl is again untreated, despite evidence (some shown below) that blood lead levels over 5-10ug/dl can increase the risk of death due to cardiovascular disease.
The next incidence chart shows something even more disturbing about Australian children.
As you can see on the world map, Australia is in a class of it’s own when it comes to ADHD incidence. The causes of this disproportionately high rate of ADHD are probably due to a lot of things, like still using insecticides, fungicides and other chemicals banned in most other non-third world counties. One of the causes could be toxic metals which are far more prevalent than we realise.
ADHD is attention deficit hyperactivity disorder. It’s a neurodevelopmental condition that is characterized by developmentally inappropriate levels of inattention, impulsivity, and hyperactivity that can cause a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development.
For a long time, clinicians thought you grew out of ADHD, but it turns out that isn’t the case because while many adults and young adults with ADHD have compensated to live fairly “normal” lives for some it has resulted in severe functional, social or occupational impairment.
We have no idea why Australia leads the world in ADHD incidence, but I do know one possible contributing cause, lead. Just like the scenario where lead exposure can cause something that looks like autism, it can also cause symptoms of ADHD. But do we test for lead exposure if ADHD is suspected?
In Australia, we treat ADHD with drugs. The psychostimulant medications mainly used to treat ADHD are dexamfetamine, Ritalin and lisdexamfetamine. These drugs have a bucket-load of potentially severe side-affects like psychoses, mood swings and even seizures, so there is significant risk involved. They also need to be taken long-term as they are not a cure.
IF some of the cases of infant ADHD are caused by lead, and removal of the lead provided a permanent cure, that would be worth doing. Why don’t we measure blood lead levels to find out, and is chelation really more risky than psychoactive drugswhere we have no idea of the other possible consequences?
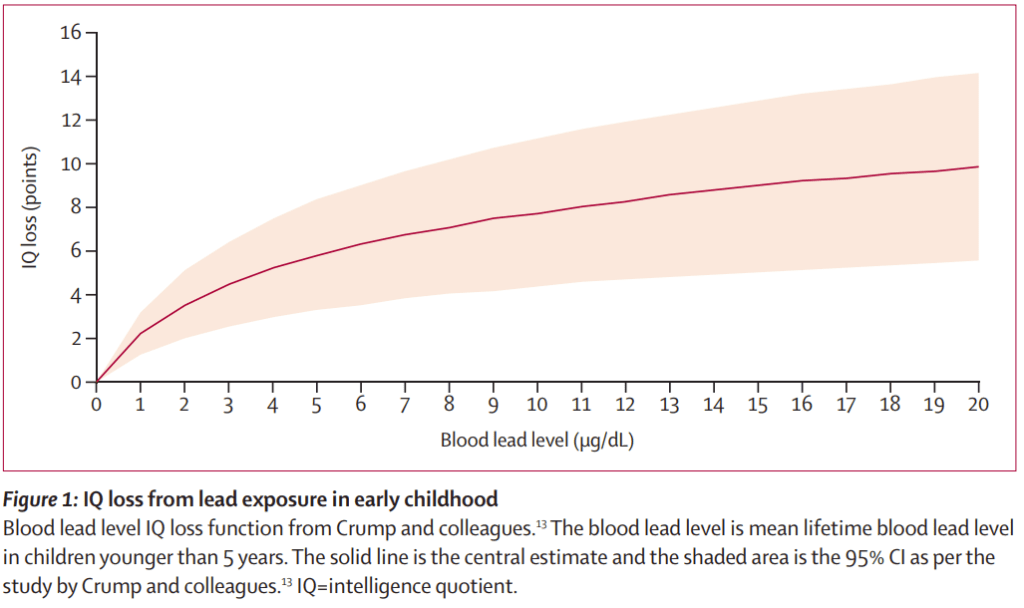
How about the other not so obvious effects of lead on infants, like a drop in IQ? I’ve shown the graph of IQ loss vs blood lead levels in an earlier blog, but here it is again (from the Lancet):
It’s hard to be more eloquent than the following article in the American Journal of Pediatric Health. I’d like to quote the complete article because it’s short and so well worth reading.
Lead Poisoning in the 21st Century: The Silent Epidemic Continues
Creating a disturbing sense of deja vu and in line with current trends of science denial, some skeptics are seeking to minimize the Flint,Michigan, water crisis and thus impede efforts to mitigate this humanmade disaster and prevent similar crises. They argue that the rise in Flint children’s blood lead levels did not warrant a state of emergency and that Flint’s kids were not poisoned. They are wrong. We represent three generations of pediatricians and child health researchers. In our professional lifetimes, we have seen repeated reductions in the levels of lead considered toxic as new research has shown time and again that blood lead levels previously considered safe are in fact harmful to children’s health. With each of these reductions, we have battled waves of skepticism from well-meaning academicians, the inertia of government agencies, and nefarious attempts by industry and their agents to undermine the science and to dismiss the increasingly clear evidence of lead’s toxic effects at ever lower levels. The science is now unequivocal. There is no acceptable level of lead. There is no safe threshold. Lead is pernicious at the lowest increments of exposure. The World Health Organization and the Centers for Disease Control and Prevention have declared that no level of lead in blood is safe. Driven by austerity and a corrosion of democracy, Flint’s public health disaster resulted in population-wide lead contamination of drinking water. In many homes it was categorized as hazardous waste. Not surprisingly, people interpret ingesting a poison as being poisoned. This definition of poisoning may not be equivalent to the toxicologist’s definition of acute poisoning, but it is poisoning and its consequences can be lifelong. This semantic nit-picking is counterproductive. There should be no disconnect between doctors who treat individual patients and public health practitioners who look at population-wide data and implications. Today, children rarely come to our emergency departments and intensive care units with symptoms of acute lead intoxication—seizing and being comatose—as they often did in generations past. However, this does not equate to no harm done. The impact of lead is insidious and often referred to as a “silent epidemic.” The effects of lead poisoning are not usually detected in a short visit with a doctor. The population impacts are, however, staggering. The consequences are one or two more kids in each classroom with symptoms of attention deficit hyperactivity disorder, 10 or 15 more kids in each school in special education programs, and fewer kids who are truly gifted. A five-point reduction in average IQ caused by widespread exposure to lead will result in a 50% increase in the number of children with IQ scores below 70 and a 50% decrease in the number with IQs higher than 130. In adults, lead exposure results in cardiovascular and kidney problems. And some studies have shown that children exposed to lead are at increased risk for school failure, unemployment, and incarceration. Now more than ever, it’s time to renew and refocus efforts to ensure that the blood of children in cities such as Flint; Detroit, Michigan; Chicago, Illinois; Baltimore, Maryland; Newark, New Jersey; Philadelphia, Pennsylvania; and beyond are never used as detectors of environmental contamination. Specifically, this means a renewed effort to update outdated action levels, remediate homes, replace lead pipes, and eliminate all the other sources of lead in our environment before our children are poisoned. That is the legacy we hope to leave the next generation.
Australia may not have a Flint Michigan where incompetent officialdom stupidly poisoned much of a small city with lead because of lead leaching out of lead pipes, but we do have areas of cities that have high levels of lead, either as a result of leaded petrol, or environmental lead, or lead pollution from the mining, smelting and transport of lead.
And we have a lot of government agencies that are pretty busy ignoring the true cost of ignoring lead poisoning. And there was the situation in Yarrabah where a broken-down pH adjuster allowed acidic bore water to leach lead out of brass fittings and lead soldered pipes. When various news services had headlines about lead poisoning in Yarrabah, the Health Minister went there to announce funding for a new pH adjuster. That was one year after the request for funding for a replacement, but it’s pretty obvious that in the absence of politically damaging news stories, it’s easier to ignore any problems.
Thanks to lead paint and a host of other sources of lead, I can state with absolute certainty that some children in Australia will be adveresely affected by lead and have their futures blighted. Let’s make a guess about how many.
There are roughly 1.5 million children aged under 4 years in Australia who are exquisitely sensitive to lead, 2.2 million between 5 and 12 and 1.4 million between 13 to 17. The US has the added risk of lead pipes in older houses, so statistics of 1 in 6 children affected by lead quoted by the CDC may possibly overestimate the number of children affected in Australia. But even if 1 in 20 children are affected by lead in Australia, that equates to about 250,000 children in Australia that are potentially affected by lead. It’s anyone’s guess if this is the case because we just don’t know thanks to the lack of testing. Talk about looking the other way!
We have all the rest of the sources of lead exposure that are seen in the USA. But there is a big difference in one area. With the possible exception of Broken Hill, there is little evidence that any government agencies are taking any active steps to drastically reduce lead exposure. It’s notable that in Broken Hill the lead exposure reductions have largely been due to local community action.
I guess it’s now time to focus on adults.
Let’s start with another graph posted earlier from the Lancet. This is cardiovascular death risks versus blood lead levels.
Notice that anything over 1 ug/dl results in an increase in the risk of death from cardiovascular disease, whether it’s atherosclerosis, peripheral vascular disease, high blood pressure causing strokes and so on.
Long term studies of the health of lead risk workers in Australia has found alarming increases in the incidence of various cancers in workers exposed to lead. As for the general population, we don’t know because just about the only people that get tested for lead are people whose occupation exposes them to lead.
If we don’t test for lead in the general population, then the authorities can also “safely” ignore the effects of lead on the general population. It doesn’t mean that people aren’t adversely affected by lead, but by not testing them, we simply don’t know. If our governments are unwilling to acknowledge the costs to our economy of doing nothing about lead, then we have a problem.
If we add up the health costs: the costs to the justice system, the loss of wages, the social costs of supporting lead-affected children, the reductions in productivity due to loss of IQ, and the economic costs of deaths caused by lead, the total amounts are enormous. And yet we (our government), continue to look the other way when it comes to lead. Are they so corrupt and influenced by lobby groups, or are they afraid to open the Pandora’s box of damage that lead inflicts on the community?
There’s really not that much more to say that hasn’t been said already. But it would be remiss of me not to point out that youth and adult violence and crime have been linked to lead exposure. The next time you hear about demands for more policing to reduce crime, maybe some blood lead testing could reveal a problem that might have a solution other than more youth detention centres.
When I was trying to tidy up the previous blog post “How to protect yourself and the people you love from lead poisoning”, a few things came together. If you’re not interested in workplace health and safety, please scroll down to the bottom of this blog post and you’ll find out how to protect yourself from lead.
My journey of learning about lead and chelation started back in 1982 with a break between then and now. In the interim I’ve learned quite a bit about lead toxicity, and the exposure to lead that all of us face, with lead risk workers on the front lines, and also how lead exposure might be something we can face without any harm.
Of all the things that bother me about the failure to properly address exposure to lead, it’s that despite knowing the harm that lead can do, next to nothing is done to alleviate the effects of lead, particularly in children. This doesn’t need rocket science, or new drugs and treatments, all it needs is applying what we’ve already got and learned in the last 60 years. Why is that too hard?
I started this blog to hopefully force, embarrass or whatever a change to the existing workplace health and safety regulations about lead risk safety monitoring. I have a relative working in Mt Isa and a conversation with him caused me to check what the regulations were. They were insane in my opinion because rather than “protecting” lead risk workers, they were doing the opposite, because they ignored the fact that the fall in blood lead levels (BLL) when a worker was removed from lead exposure wasn’t due to lead leaving the body, which it doesn’t for the most part, but was due to lead moving elsewhere in the body, like soft tissues including the brain, and finally to bone. Lead mimics calcium in the body, and like calcium, it’s retained in the body.
An absolutely beautiful example of how little progress there has been in the workplace health and safety (WHS) are when it comes to lead risk workers is this 1980 US OHSA incident report which uses regulations that are still in place today:
Lead is eliminated from the body via urine and feces. NIOSH recommends that a blood lead value of 60 micrograms per 100 grams whole blood (60 ug Pb/100 g blood) be the maximum occupational blood lead level. When this value is exceeded, the employee should be removed from the lead exposure to allow his body to reduce its lead burden.
Here we are 43 years later, and the BLL level for lead risk worker removal is still only half of what it was in 1980 and is still based on the absolutely inexcusably stupid assumption that lead rapidly leaves the body when we’ve had 43 years to correct that error. Would any organization that cared about worker safety ignore a basic problem for 43 years?
Removing a worker with a BLL over 30ug/dl from exposure doesn’t do a damn thing to reduce the body burden of lead. Removal is not a protective action. If anything, it’s a penalty applied to the employer which may in fact not be inappropriate. There are minor losses of lead when red blood cells containing lead are broken down, but the bulk of the lead is there for decades, maybe your whole life.
Your’e probably sick of seeing this diagram, but it’s a great way to illustrate where you are with a BLL over 30ug/dl, pretty much screwed.
At about 15ug/dl, you’re seeing all the sub-clinical symptoms that indicate excessive lead exposure. At 30ug/dl, you see increased blood pressure, increased rates of cancer, a doubling or trebling of the risk of dying of cardiovascular disease. Simple stuff.
The problem was so obvious to me that I stupidly assumed that if I explained what was wrong in a simple enough way, people would realise that they were harming workers and do something to fix the problem. After all, that’s the role of people in WHS isn’t it? They’re supposed to protect workers and promote a safe work environment?
Wrong. Think about the role of HR (human resources). They’re not there for the benefit of the workers, they’re there to manage the workers on the bosses behalf. WHS is there to do the minimum amount they can within the regulatory framework defined by government agencies. The easy stuff gets done, the more complicated stuff like biohazard monitoring, has to appear as if something is being done, even if it results in harm to workers.
I’ve yet to encounter an organization; Glencore, Resouces Safety and Queensland Health, or Safe Work Australia, that did anything but pass the buck. Mt Isa Mines or Xstrata, before Glencore took over, might have done something but we now have Glencore. Glencore don’t seem to want to know, especially since there’s another little issue arising in Townsville where Mt Isa has been shipping lead ingots and concentrates for the last 90 years.
In the case of Safe Work Australia, they’re quite happy to admit that there are problems with lead biohazard management in their documentation, but that concern isn’t reflected in their model regulations which are the basis of regulations used by all the states (and NT) except Victoria. The existing lead risk worker “safety” regulations use lead risk workers as “mine canaries”.
Lead risk worker safety, or more correctly protection from harm, is obviously too difficult to even consider. RSHQ (mining WHS, Queensland) has a logo that says “ZERO SERIOUS HARM”. Considering the serious harm lead can cause in lead risk worker’s bodies, and not even considering if one of them is a female of child-bearing age, this logo is a blatant lie if it represents RSHQ stated aims, and a bad joke regardless.
I’ve said all this before in other posts, but why bring it up again now?
Well, it’s because things could be even worse.
I started looking at some of the international WHS sources, and I came across a section of the US Occupational Health and Safety Agency standard about lead “safety” that nearly blew my mind. As you’d know I’ve been proposing chelation to remove lead as a solution to avoid the ill effects of lead. The OHSA documentation t basically absolutely disallows using chelation therapy for anything but severe lead poisoning.
I’d like to quote some of it below (the bolding is mine):
The medical surveillance section of the standard also contains provisions dealing with chelation. Chelation is the use of certain drugs (administered in pill form or injected into the body) to reduce the amount of lead absorbed in body tissues. Experience accumulated by the medical and scientific communities has largely confirmed the effectiveness of this type of therapy for the treatment of very severe lead poisoning. On the other hand, it has also been established that there can be a long list of extremely harmful side effects associated with the use of chelating agents. The medical community has balanced the advantages and disadvantages resulting from the use of chelating agents in various circumstances and has established when the use of these agents is acceptable. The standard includes these accepted limitations due to a history of abuse of chelation therapy by some lead companies. The most widely used chelating agents are calcium disodium EDTA, (Ca Na2 EDTA), Calcium Disodium Versenate (Versenate), and d-penicillamine (pencillamine or Cupramine).
The standard prohibits “prophylactic chelation” of any employee by any person the employer retains, supervises or controls. Prophylactic chelation is the routine use of chelating or similarly acting drugs to prevent elevated blood levels in workers who are occupationally exposed to lead, or the use of these drugs to routinely lower blood lead levels to predesignated concentrations believed to be “safe”. It should be emphasized that where an employer takes a worker who has no symptoms of lead poisoning and has chelation carried out by a physician (either inside or outside of a hospital) solely to reduce the worker’s blood lead level, that will generally be considered prophylactic chelation. The use of a hospital and a physician does not mean that prophylactic chelation is not being performed. Routine chelation to prevent increased or reduce current blood lead levels is unacceptable whatever the setting.
The standard allows the use of “therapeutic” or “diagnostic” chelation if administered under the supervision of a licensed physician in a clinical setting with thorough and appropriate medical monitoring. Therapeutic chelation responds to severe lead poisoning where there are marked symptoms. Diagnostic chelation involved giving a patient a dose of the drug then collecting all urine excreted for some period of time as an aid to the diagnosis of lead poisoning.
Why would any authority consider that chelation treatment to remove lead is only justified at the point where gross injury is likely and for no other reason?
There were a number of clues, but the comment about the history of abuse of chelation therapy was the key. What was that about?
It seems that some lead companies tried using chelation therapy as an excuse for not having to reduce lead exposure in the work environment, and some other companies genuinely tried to reduce the amount of lead in workers bodies with well monitored and supervised chelation therapy in hospital.
I can understand that the first example, which didn’t work incidentally, could cause concern. It’s important to limit exposure to lead as much as possible and not bothering to do that is pretty blatant. But I do understand the logic since chelation is a lot less expensive that equipment to minimise lead dust production and exposure.
But medically supervised monitoring and treatment to remove lead? Isn’t that a positive move?
Apparently not. “Routine chelation to prevent increased or reduce current blood lead levels is unacceptable whatever the setting.“.
Okay, so this is a bit like saying we can test for the presence of cancer, but we can only attempt to treat it if it’s stage 4 cancer. Really?
If you read this review article: (Royce S, Rosenberg J: Chelation therapy in workers with lead exposure. West J Med 1993 Apr; 158:372-375), you might start to understand what the nonsense in the OHSA standard is all about. I can’t help pointing out that the authors don’t appear to have understood what they were talking about when it comes to chelation, though that’s fairly common. The comment “Evidence that chelation therapy with edetate calcium disodium is ineffective in treating atherosclerosis led the California Medical Board to consider this practice unacceptable.” While removing lead in a timely fashion may have prevented atherosclerosis, removing calcium plaques from arteries uses the same form of EDTA as treating patients with hypercalcemia, Disodium EDTA. Calcium disodium EDTA will NOT remove any calcium form the body. Surely anyone writing a review about chelation would know that. If they don’t, they shouldn’t be commenting on chelation.
The scary part is this review is used as a basis for decision-making by OHSA. Ignorance feeds ignorance, it seems.
Then “Chelation initially lowers blood lead levels and therefore may decrease the length of time an employee must be away from lead exposure and provided medical removal protection benefits under the OSHA standard. Employers may thus be encouraged to rely on chelation rather than instituting controls to prevent lead exposure.
Treatment using chelation agents represents the failure to prevent lead overexposure and should trigger further follow-up. Physicians caring for workers with elevated blood lead levels can play a key role in identifying others at risk and in prompting actions by workers, employers, and governmental agencies to control lead exposure in workplaces.
This review provides the justification for the latest OHSA standard.
But let’s repeat that statement, “Treatment using chelation agents represents the failure to prevent lead overexposure“. In the context that chelation and the benefits of removal of lead is ignored, this almost makes sense. But in the context that the amount of lead in a lead workers body is constantly increasing to the point where serious symptoms WILL occur, it is utter nonsense.
One last gem: The routine use of chelating agents to prevent rises in blood lead levels or the development of symptoms is considered “prophylactic chelation” by OSHA, which prohibits such practice by any person retained or supervised by lead-using employers, and constitutes inappropriate medical practice.
In the US lead industry, environmental monitoring, blood lead monitoring and removal from lead exposure if overexposure happens, are the ONLY mandated and allowed safety provisions implemented for the safety of lead workers. Workers are treated by chelation only when there is an imminent risk of gross injury including death from excess lead exposure.
We need to put the OHSA standard’s comments about prophylactic chelation into a historical perspective by presenting data that makes a mockery of the present-day standard. I’ve found a 1962 paper (Williams JD, Matthews GA, Judd AW, Oral Calcium Disodium Versenate in Treatment of Lead Poisoning , Br J Ind Med. 1962 Jul; 19(3): 211–215.) This presents a study of the effects of oral calcium disodium EDTA (also called Versenate) in workers suffering lead poisoning. It provides a good review of previous work, but more importantly, it indicates the safety and effectiveness of oral EDTA.
And yet, 60 years later, OHSA have effectively banned chelation for anything but severe lead poisoning because chelation upsets their view of how things should work. ”They follow orders as they were told to and will not allow exceptions”, like the Vogons in “Hitchhikers Guide to the Galaxy”.
This is what we have looking after the safety of lead workers.
It would give me great pleasure to be able to say things were better in Australia, but I’m not sure I can. The existing Australian WHS regulations, while not banning chelation, don’t protect workers from the long-term effects of lead poisoning either. What is it about bureaucracy that can make human lives irrelevant?
I’ve called lead poisoning a silent epidemic, and it’s silent because there is SBA (no that’s not a misspelling) testing of lead in the general population (no-occupational lead exposure) and unless you present with a blood lead level of over 45-70 ug/dl (lower value for children) you will not get treated to remove lead, regardless of the fact that damage due to lead (for example) neurological symptoms, blood pressure increases and so on happen at levels below 10ug/dl.
I would encourage you to read the very short article “Lead Poisoning in the 21st Century: The Silent Epidemic Continues”, (Hanna-Attisha M, Lanphear B, Landrigan P, Am J Public Health. 2018 November; 108(11): 1430). It was written by 3 concerned pediatricians about the situation arising in Flint , Michigan. I should be concentrating on WHS issues, but I can’t help reminding you that lead affects everyone.
I’ll quote a section out of this article:
The consequences are one or two more kids in each classroom with symptoms of attention deficit hyperactivity disorder, 10 or 15 more kids in each school in special education programs, and fewer kids who are truly gifted. A five-point reduction in average IQ caused by widespread exposure to lead will result in a 50% increase in the number of children with IQ scores below 70 and a 50% decrease in the number with IQs higher than 130 and some studies have shown that children exposed to lead are at increased risk for school failure, unemployment, and incarceration.
I’ll display the relevant chart yet again:
Where do you draw the line and start doing something to halt the inevitable increase in blood lead levels or to remove the lead? How much damage does there have to be before someone takes notice? When are we finally going to redefine what clinical symptoms mean so we avoid this harm?
Our authorities are either dangerously ignorant, or they’re so influenced by the lead industry that they are deliberately ignoring the impact that lead exposure has; the health impact, the educational impact, the impact on our justice system and the overall huge economic cost to Australia.
Sure, we need the mining royalties, but why do ordinary Austrlians have to give up their health and maybe even their lives because of the lack of action about lead.
The inquiry into the Cadia mine dust problems is an example people should consider, as is Queensland Health no longer providing information on notifiable lead tests or the NHMRC recommendation against wide-scale blood lead testing which is so desperately needed so we can properly understand the scope of our epidemic of lead.
One thing is obvious, in the case of both the US and Australia, and that is that occupational health and safety, or workplace health and safety, are not there to ensure a safe work environment for workers when it comes to lead biohazard management. The are there to make sure the often broken rules are enforced. In reading the Safe Work Australia documentation, you can’t avoid the impression that things are more about the employers than the workers, and appearing to be doing something. Since not even the unions that used to be involved in the mining industry have shown any interest in this tragedy of errors, what do we do?.
I wrote that there was an enormous economic cost involved in ignoring lead exposure, and in an earlier post I pointed out the Australia is grouped with other third world counties when it comes to our dependence on mining, and the influence of the miners. We need the money and jobs, and I’m okay with that, as long as people don’t have to give up their health and their lives in the process. We can deal with the dangers of lead if we try. We absolutely have the knowledge and experience to protect people.
But that’s not what happens. Why?
Anyway, scroll down to learn how to protect yourself from lead, because if you don’t protect yourself and your loved ones from the effects of lead, I can assure you that no one else is likely to do it.
I thought I’d write this to put together a guide of sorts on how to avoid lead poisoning in a lead-rich environment. The lead-rich definition is fairly broad because it includes occupational lead, environmental lead, whether natural or due to lead pollution and things like lead paint on old (pre-1970 construction) buildings and even old buses and cars. It includes lead pollution from old car batteries, lead flashing on roofs, lead solder on old water tanks and a lot more.
It’ll take a while to complete this guide so please understand it’s a work in progress. As for me, I’m retired, but I have a PhD in Medicine, spent 14 years in medical research studying aspects of metal metabolism in animals and humans, and I have had the luxury of spending a lot of time finding out as much as I could about lead. What I’ve found is frightening, but it’s pretty clear that the effects of lead can be minimized or avoided, which is kind of why I’m writing this.
INTRODUCTION
Broadly speaking the first thing you need to appreciate is just how subtle and dangerous exposure to lead can be, and how long it can take before you get significant symptoms that are recognized as due to lead exposure. While you’ll get pretty obvious symptoms if you cop a large dose of lead, it takes a long time for anything but neurological symptoms to show up.
Insomnia, loss of appetite, decreased libido, depression, irritability, memory loss and headaches just aren’t seen as symptoms of something like sub-clinical lead poisoning. You can also get neurological symptoms that look like MS, or Parkinson’s or dementia but you can bet they probably won’t test for lead either.
If you’ve got young children, then I would strongly suggest you get and read a copy of Nancy Hallaway’s kindle e-book (From Amazon, $8), “Autism, ADD, or Lead Poisoning? Turning Lead into Gold”. It will frighten you, but also give you an appreciation of the potentially devastating effects of lead on young children. It will also inform you that at least some of the deleterious effects of lead are reversible, and that’s a theme I will bring up again and again. While some of the effects of lead are irreversible, some aren’t.
Also take the time to watch Ralph Spezio’s YouTube video (https://www.youtube.com/watch?v=mSwHSE6_ZoI) because it will absolutely put things into perspective for you about what lead exposure can do to children. Ralph Spezio is talking about relatively low levels of lead, around 10ug/dl which have been detected in a reasonable percentage of children tested in Mt Isa, as an example. This video could be about your kids!
Lead is dangerous when it gets into your body. Lead ore dust , often lead sulphide (galena), is an insoluble form of lead. But if the dust gets into your body, it gets converted into a soluble form of lead which is avidly taken up into your body. Organic acids like vinegar are a great way to make lead soluble. Lead acetate used to be called “supa” by the Romans and was used to sweeten food and wine.
Adults will absorb up to 10% of ingested lead, infants up to 40% of the lead because of a greater need for calcium. The mechanisms that handle calcium uptake and deposition, do the same with lead.
Lead accumulates in the body as exposure continues and very little leaves your body unless something like gestation or breast-feeding liberates calcium and therefore lead from the mother’s body to her baby. That’s not giving your child a very good start in life and in my mind represents the absolute worst case scenario, a child born with lead poisoning.
The accumulation of lead is called bioaccumulation and most of the lead you absorb will end up in your bones, with some in teeth in infants and a good bit in your brain. As the total amount of lead stored in your body increases so do disease states caused by lead, especially neurological diseases.
In the USA the CDC estimates that there are up to 400,000 lead comorbidities every year, that is deaths where lead was a contributor. There’s little reason to think the situation in Australia is much better. There could be up to 35,000-40,000 Australians a year dying because of the effects of lead. I bet you weren’t aware of that possibility. Didn’t they tell you?
The effects of lead in infants is much more extreme, partly because of the higher intake of lead, and partly because the developing brain is much more susceptible to the effects of lead. Relatively low levels of lead, below the notification point where our health authorities are “supposed” to take some action, still have profound neurological effects. Miniscule (nanomolar) amounts of lead in an infants brain will affect their learning capacity and behaviour.
The CDC also estimates that 1 in 6 children the in the US are affected by lead. There’s little reason to think the statistics in Australia are that much better because we have no data on the incidence of raised lead levels in the general child population.
Things could even be worse in Australia because unlike the US, non-occupational blood lead testing is discouraged. It is likely that less than 1 in 2000 (that’s 0.05%) of the general population has been tested for lead exposure. If you don’t test for lead, you won’t find it.
We have multiple problems in our medical services: a lack of wide-spread awareness of the dangers of lead, a lack of appreciation of the contribution of lead to disease processes, a lack of appreciation that excess lead can and should be safely removed and as a result, a lack of testing for the presence of lead.
We had nearly 50 years of being told that leaded petrol was safe, and while we mustn’t discount the influence of the mining companies, and bureaucratic inertia, I’m sure that’s a factor in the lack of appreciation that lead represents a massive public health failure.
It’s a sad reality that we probably can’t depend on our politicians or medical services to protect people from the medical outcomes of lead exposure. Even the workplace health and safety organizations get a big FAIL when it comes to protecting lead workers from lead biohazards. In the absence of due care and in the presence of almost criminal negligence, we’re left with the reality that we have to take care of ourselves when it comes to lead.
There are 3 parts to protecting yourself from lead; detecting what is lead-contaminated, reducing exposure as much as possible, and where exposure is unavoidable, doing something to remove the lead before it does permanent harm.
Part 1 – Lead Detection
If we stick to talking about stuff that’s relevant today, then there are 3 technologies that are suitable for detecting lead contamination.
The first is ICP-MS, inductively coupled plasma mass spectrometry. ICP-MS can be used to measure lead (and other heavy metals) content in blood and just about anything else provided it is digested in acid beforehand. It is very sensitive and there are many pathology and analytical services with ICP-MS.
Blood lead levels (PbB or BLL) are measured using ICP-MS and the cost of the test is a bit over $30. Medicare actively discourages blood tests unless there are symptoms suggesting lead exposure. That little gem comes thanks to a 2015 NHMRC report that recommended against widespread blood lead testing and so the smart people at Medicare will do things like threaten to rescind a doctor’s Medicare provider number if he orders any “unnecessary” blood lead tests. Of course, if you’re willing to pay the $30 yourself, there’s nothing stopping you getting your doctor to send a blood or urine sample to an analytical or pathology lab for lead testing.
If you want to find out the lead content in something like paint, or soil samples, then the traditional way to do that is send the sample to an analytical lab, pay your money and get the results of chemical measurement of lead. Chemical estimation of lead has probably mostly been replaced by ICP-MS, but it’s still out there.
You can get personal lead test swabs, which are inexpensive ($18 for 30 on eBay) but they’re really only intended for relatively high levels of lead, like that found in lead paint. But if the test swab does detect anything, it’s serious.
The third way to measure lead is relatively new from the viewpoint of affordability and medical use. It’s X-ray fluorescence spectrometry (XRF) and it works by exposing a sample to a small amount of x-rays, and measuring the fluorescent x-rays given off. XRF is fast, noninvasive and is extensively used in the mining and metallurgy industry because you can determine things like alloy composition. Once it’s calibrated, anyone can potentially use an XRF like an oversize infrared thermometer, but XRF gives you metal content, not temperature.
XRF is also used in a lot of other scenarios, for example by Curtin University researchers to measure lead levels in wildlife, in the Vegesafe program that tests soil, and even at Taronga Park Zoo where it is used to determine an animal’s provenance by looking at a fingerprint of metals.. XRF spectrometers can be hired in Melbourne and Perth to test for things like determining the concentration of lead in auto paint.
There’s an interesting lady, Tamara Rubin, who has a website LeadSafeMama (https://tamararubin.com) where she posts the results of testing the lead content of just about anything with her own personal XRF spectrometer.
XRF can also be used to measure the amount of lead in bones. Recent work by researchers at Purdue University have used a special portable XRF spectrometer that’s been calibrated to estimate bone lead. Remember that up to 95% of the lead in your body ends up in bone, so measuring bone lead gives you a pretty good idea of the amount of lead in your body and the risk to your health.
XRF is a game-changer for reducing exposure to lead because if you have access to one, YOU can measure the amount of lead in whatever you want. In the dust in your attic, the soil in your garden, where your kids play and so on.
Imagine being able to identify any lead hazards yourself without having to depend on an external testing lab or external agencies.
Maybe your community could crowd-fund an XRF Spectrometer. Contact Tamara Rubin (Tamararubin.com) for advice on her collaborative community project to fund getting an XRF spectrometer.
2. Protection
If you live in a lead-rich area, either due to natural ores or pollution, or near a mine, lead ore dust is an inevitable part of the environment. The dust will contaminate your water tanks, lead will contaminate the plants you grow in lead-contaminated soil and lead will contaminate animals that are raised on lead contaminated soil.
There are suburbs in Melbourne and Sydney where lead contamination due to leaded petrol means it’s not safe to eat the vegetables you grow. There are cattle stations in North Queensland that had their cattle rejected for live export to Indonesia because of high lead levels. Cattle for export now have their lead removed and I dearly hope that happens for cattle for domestic consumption as well. There are new housing developments in areas that are likely lead-contaminated, like the sites around old lead smelters.
We need strategies for dealing with the dust, for getting lead free water and vegetables, and hopefully doing the same for our food animals.
The Living with Lead alliance in Mt Isa instigated a program where particularly contaminated yards were concreted over, with articial turf on top. But that’s not really a terribly practical solution.
Keeping your houses relatively dust free helps a lot, but adding an air purifier in the house to reduce circulating dust in the air, wearing dust masks when doing anything that raises dust, like mowing the lawn, are all useful.
Another interesting strategy that is used for lead (and other heavy metal) neutralization in industry is a chelating agent called TMT (1,3,5 trimercapto 2,4,6 trazine). TMT is used to wash flue gases in some smelters to bind to lead and form an almost inert complex that is apparently biologically inert. There might be quite a market in a commercial cleaning product ontaining TMT, named something like “Get the lead out”.
If you have a pre-1970s house, the paint can be hideously dangerous to children because lead paint has a sweet taste that is irresistible to children and animals. Licking paint has killed children in the past. It’s incredibly nasty. At least some of the older public housing in Mt Isa has lead paint, and yards full of lead paint dust and chips from flaking paint or sanding.
My aunt has an old house that was covered in lead paint. I’ve never approved of PVC siding, but if it covers up lead paint, it’s more than acceptable. Have I stressed that lead paint is really dangerous?
The data from the testing programs is shared as part of a global environment mapping effort (Map My Environment: Global (shinyapps.io)), which would be wonderfully subversive for your group if you can get enough local residents to take part.
If raised levels of lead are detected, then here’s what to do.
Water from rain water tanks needs special attention because the pH of the water will influence lead bioavailability as will any bacteria in the sludge at the bottom of the tank. Some of the lead in rainwater is still in the form of dust, some may have been converted to soluble lead by microbial action.
I’ll quote part of SA Health’s commentary on lead in rainwater in Port Pirie where lead contamination is still all too common:
Rainwater in Port Pirie contains lead. Studies have shown that contamination can be at levels high enough to cause serious health concerns or poisoning if drinking rainwater or using it in any circumstance where the end product is consumed. This risk can be easily avoided by drinking and using mains or bottled water.
Drinking contaminated rainwater is one of the ways lead can enter your body. Together with other exposure sources around Port Pirie, consuming rainwater can cause elevated blood lead levels, often above the National Health and Medical Research Council (NHMRC) recommended exposure investigation level of five micrograms per decilitre (μg/dL).
Pregnant women and young children should not use or drink rainwater collected in Port Pirie.
Once you filter out the lead dust, which is relatively easy, the least expensive way to remove soluble lead is with an ion exchange column (mixed bed, cations and anions) or cation (metal ions only) . This YouTube video shows how to deal with mixed ion exchange resin ( https://www.youtube.com/watch?v=Zij-PwFHvBA). A cation exchange column can be more easily regenerated with hydrochloric acid. A colour-changing resin would let you know when it needs to be regenerated (Deep Green Cation Ion Resin CSP10 – A&C Pure Water Treatment (ancpurewater.com)
Reverse osmosis will remove lead as well and it has a higher water throughput. Depending on your needs this may be a better choice, but it’s also more much expensive. There is some evidence that zeolites remove lead but I haven’t got all the relevant information.
Rain water, lead or not, has relatively few salts so if you’re used to drinking rain water the lack of salts won’t bother you. Otherwise ,you might want to add some salts to the purified water for taste. In any event, an occasional metal/salt supplement isn’t a bad idea in any case.
Lead in food is a challenge if the soil is contaminated.
If your soil is contaminated with lead, you need to realise that lead paint on a pre-1980s house that has been renovated, will have contaminated the whole area around the house. Lead dust is a minor contributor to the contamination in this case. Growing vegetables in raised garden beds filled with clean soil is the best safe option if soil in your garden is found to be contaminated.
Another option is hydroponic vegetables if you want to avoid any risk of lead contamination AND you have lead-free water.
Lead in animals is harder yet. The example I gave earlier about cattle in North Queensland had a relatively easy solution, The cattle are kept in a feedlot and fed a chelating agent, TMT, and after a few weeks they test free of lead and away they go. As mentioned earlier, TMT is an industrial heavy-metal chelating agent.
Use geofabric as a base for clean soil or sand for your chicken run and you can avoid lead-contaminated eggs.
It’s worth pointing out that animals are also adversely affected by lead. Not as much as humans but that’s because we live longer and can accumulate more lead. I have a story about cattle in a large paddock that also contained an old bus. The cattle weren’t thriving and even after the local veterinarian got involved, nothing was found to explain why the cattle were sickly. Until one day when the farmer spotted one of his cattle licking the old bus. It turns out the bus was painted with lead paint, and when the bus was removed, so did the problems.
But back to what you can do. If you can remove lead that you’ve eaten and absorbed, then that’s nearly as good, and a lot easier, than trying to make your food and environment lead-free. If I was offered a prime eye fillet from North Queensland, I’d enjoy it regardless of whether it contained lead or not because I’ve taken an oral chelating agent.
That’s kind of like a doctor I knew that had type 1 diabetes. When faced with a fabulous dessert, he’d mentally estimate the amount of sugar and inject an appropriate amount of insulin. You can have your cake and eat it too.
3. Lead Removal
This is the big kahuna of dealing with lead using a molecule that specifically forms complexes with metal ions, called a chelator, or chelating agent. A whole lot of things will bind metal ions, but chelators are generally much more specific.
Chelators are used as food additives to reduce spoilage and oxidation, they are used to remove heavy metals from smelter flue gases, and heavy metals from animals and humans.
I’ll give an example.
Lewisite was an arsenic-based chemical warfare agent invented by the British in 1918, too late to be used in WW1. British anti Lewisite (BAL) was developed in 1940 as an antidote and pre-treatment in case Lewisite was used and blown into the allied trenches. Thankfully, Lewisite was never used but BAL turned out to be incredibly useful to treat arsenic poisoning and as such was the first medically used chelation agent. It’s still in use at times.
There are many other chelators, relatively specific for other heavy metals. A number of sulphur-containing chelators work well for removing lead but the most common one in use is EDTA (ethylenediaminetetraacetic acid). EDTA was invented in 1935 but it was first used in the dye industry and as an anticoagulant and subsequently for the treatment of hypercalcemia and eventually lead poisoning.
In the 1950s and 1960 researchers noted that EDTA treatment for lead poisoning also improved vascular disease, causing a huge interest in using EDTA to treat all sorts of cardiovascular problems. With everyone using EDTA and no proper protocols, it was inevitable there would be fatal accidents. Things got so uncontrolled that the use of EDTA was actively discouraged to the point of chelation therapy being banned by some states in the US. The cases of renal damage occurred in the 1950s, the child dying of hypocalcemia was a case of ignorance and negligence, using too high a dose of the wrong form of EDTA.
In 1989, a “Protocol for the Safe and Effective Administration of EDTA” was developed and subsequently updated. The detailed protocol provides strict criteria for patient selection and cautions clinicians to perform an initial evaluation of renal function and to frequently monitor renal function throughout a series of chelation treatments. Emergency procedures are outlined should adverse reactions occur.
The present-day chelation protocols used for the last 30 years or so have been proven to be safe. As I pointed out before, chelation is used to make cattle safe to eat.
But, despite an abundance of current evidence showing that chelation therapy was safe, it has kept it’s stigma in most the Medical industry, being used only when absolutely necessary. If you suffer from severe lead poisoning, then chelation therapy is used. Otherwise it is discouraged, albeit for no good medical reason. With the possible exception of essential metals depletion which can be managed with metal supplements, chelation is safe.
It’s a personal theory of mine that the effectiveness of EDTA chelation therapy threatened the livelihoods of cardiac surgeons, manufacturers of stents and drug companies who make statins, but that’s just a theory to explain why so many otherwise intelligent people would criticize something so useful.
Chelation therapy is now used as a standard treatment for treating any heavy metal toxicity in many parts of the world, but not in Australia for the most part. Then again, the amount of testing for lead and other heavy metal exposure in Australia is minimal. If you’re able to find a clinic that tests for heavy metals and removes them with chelation therapy you’ve been lucky.
Chelation works.
But however useful and safe IV chelation therapy with EDTA might now be, it’s really not all that practical in the general population because of the lack of availability from public medical services and lack of support (no rebate) by Medicare. IV chelation in Australia is quite expensive if you’re not suffering from hypercalcemia or toxic lead poisoning in the public hospital system.
Oral chelators are a better choice since taking a capsule is relatively less complicated and removing lead from bone is a slow process in any case, better suited to smaller doses over a longer period.
Of the oral chelators available that remove lead effectively, I would like to opt for calcium disodium EDTA. DMSA (Dimercapto succinic acid) is probably somewhat more effective because of it’s higher oral absorption and faster removal of brain lead, but it’s 25x more expensive and the TGA has only accredited it for veterinary and radiochemical use.
From an cost viewpoint you can buy 1kg of calcium disodium EDTA powder (food grade) for about $60+freight from bulksupplements.com. That will let you fill a bit over 1600 size 0 capsules. You can buy 2000 empty size 0 capsules which will hold about 600 mg (gelatin $40, enteric coated $92) and a size 0 capsule filling machine ($40) from buyemptycapsules.com.au. The enteric-coated capsules are liable to give you better absorption because stomach acid reduces EDTA salt solubility.
A daily dose of 6oo mg of EDTA will cost you a bit over 13 cents a capsule (enteric coated). You’ll have to fill them yourself, but that’s not too hard with the filling machine (I managed) and it’s a LOT cheaper than buying EDTA capsules online.
That one capsule a day could potentially stop any further accumulation of lead, and might even reduce the amount of lead in your body (albeit slowly).
When I was first looking for current evidence supporting oral chelation, I found a lot of case studies, but nothing relevant to lead-workers. It turns out I didn’t look far enough back. I found a gem, (Williams JD, Matthews GA, Judd AW, Oral Calcium Disodium Versenate in Treatment of Lead Poisoning , Br J Ind Med. 1962 Jul; 19(3): 211–215.). This presents a study of the effects of oral calcium disodium EDTA (Versenate) in workers suffering lead poisoning. It provides a good review of previous work in the 1950s, but more importantly, it indicates the safety and effectiveness of oral EDTA, 60 years ago.
The study used a total of 4 grams of calcium disodium EDTA per day, but my opinion is slow and easy will do a better job of removing bone lead and avoid the trace metal depletion issues discussed below.
The following diagram shows the range of lead concentration that is linked with various blood lead levels.
An argument against “prophylactic” lead removal has suggested it is unethical to give someone a “drug” unless they have disease symptoms. And yet how many times have you heard of people being prescribed prophylactic antibiotics, just in case. In any event, if you’ve been exposed to lead or are in a lead-rich environmrnt the symptoms are there, they just haven’t been diagnosed yet.
Look at the diagram below and work out which of the central nervous system symptoms are solely indicative of lead poisoning.
You’ll need to make up your own mind, but that is why there isn’t a standard protocol for oral chelators used prophylactically to prevent lead accumulation.
There are many case studies over many years that used oral chelators effectively and safely to remove lead, but not THE double-blind study that the clinicians insist they need before they’ll change their minds.
But lets run the numbers.
Calcium disodium EDTA is absorbed relatively poorly because of stomach acid, and only about 5% (using C14 labelled EDTA) enters your body. It should be absorbed more effectively if administered in enteric capsules, but let’s stick with that published 5%. If we have a dose of 600mg in a size 0 capsule, then about 30 mg should be absorbed. Calcium disodium EDTA has a molecular weight of 375, and one EDTA molecule will bind one atom of lead (molecular weight 207). That means that 30 mg can theoretically bind and remove (207/375×30) 16 mg of lead. That’s not bad considering that if you ingested 16 mg of lead and you weighed 100kg, your blood lead level would be well over 20ug/dl.
It would be safe to say that you would probably no longer be adding to your lead stores, and that’s pretty good. Always, provided you’ve minimised lead exposure as well, you should be starting to remove lead already in your body.
There are some cautions about regularly taking calcium disodium EDTA. EDTA binds other heavy metals, which is an absolute bonus if you’re a bit older and had mercury amalgam fillings in your teeth, or were using organophosphate insecticides in the past or like seafood (with heavy metals). But EDTA potentially also binds essential metals like magnesium and zinc which can then be depleted. Not a lot because the affinity for lead is greater, but a regular trace metal or zinc and magnesium supplement would be a good idea. Oral EDTA largely leaves the body within a day so a regime where you took EDTA for 6 days and a supplement on the seventh would pretty much keeps things working as needed.
We use calcium disodium EDTA because it exchanges calcium for lead and actually augments the calcium in your body. I’ve read that EDTA will also bind iron. It’s extremely unlikely EDTA will remove iron from your body, I know because my medical research included studying iron uptake. BUT, it could prevent the uptake of iron from your food. That’s great if you’ve got Haemochromatosis but not so good if you’re iron deficient. If you were to take EDTA and ferrous folate, as an example, on alternate days, that would sidestep that issue. EDTA ought to be totally cleared from your body within a day.
If you’re afraid the EDTA will stop you absorbing any of the food grade iron filings added to your favourite breakfast cereal, I can assure you that very little elemental iron is absorbed in any case, so EDTA most likely wouldn’t make any difference. If you’re a Vegan, I’m sorry to report that you won’t find many sources of bioavailable iron. That includes the fairytale of iron in spinach.
In summary, provided you manage potential essential trace metal depletion, oral calcium disodium EDTA is safe. In my book if you’ve got demonstrable lead on board (take 1 capsule, take a 12 hour urine sample and get it analysed)., you have absolute proof of lead that needs to be removed.
That’s it for now, more to come as I find time.
There is a lot more information in the many blog posts below so if you’ve got time, PLEASE READ THEM because you’ll learn a lot more they didn’t tell you about lead.!
Gross negligence refers to a person’s or organization’s conduct where an act or failure to act creates an unreasonable risk of harm to another because of the failure to exercise slight care or diligence.
That definition raises some interesting issues with regard to lead exposure.
If a business becomes or is aware of a situation that is causing harm to it’s employees, is stating that they are following all the rules enough? It can be argued that in the face of an honest and reasonable belief that all regulatory mandated procedures are being followed, then the actions are not negligent.
But we have evidence in documentation from Safe Work Australia (SWA), as well as many other sources, of lead bioaccumulation. Even the reference book for occupational workplace hazards, “Hunter’s Diseases of Occupations”, states quite clearly that lead accumulates in the body and most of it ends up in the bones.
I brought this fact to the attention of Glencore and of Resouces Safety and Health Queensland (RSHQ). Both organizations fell back on the defense that they were following the regulations provided by RSHQ or the regulatory model provided by SWA. I guess that’s fair enough at one level, except that BOTH organizations make claims about how they care about the safety of workers. Where lead biohazards are concerned they don’t care.
But if they are no longer ignorant of the flaws in the regulations that fail to deal with the continued accumulation of lead in lead risk work and the increasing risk of inevitable harm to lead workers, then they have no credible defense in the face of a claim of negligence.
If anyone reading this is a bit upset by the thought of the potentially deadly legacy they are carrying in their bodies due to their lead risk work, I am happy to provide you with copies of the documents from both organizations and copies of my emails and letters informing of your health risks. It is probably easier to make individual claims of negligence because they are likely to be settled out of court, but that’s your decision. The only point of a class action is to bring something to the public notice, and make legal firms a lot of money at your expense, but it might be worth while to force a change.
To the people with children that may be affected by lead, the course of action is reasonably simple, but you’ll probably be finding a different organization liable for negligence. The recent case of Seaton vs MIM (Glencore) showed quite clearly that most reasonable measures to minimise lead contamination in Mt Isa have been made.
The efforts are hardly as good as they could be, since Broken Hill managed to reduce infant exposure by 65%. But it’s pointless to try and blame Glencore, UNLESS you’re a female lead worker and you’ve had a child while or since working in Mt Isa. In that case, Glencore’s negligence can be proven because the lead in your body has been passed to your child in utero or by breast feeding. A safe way to measure a child’s lead burden is something called a chelation challenge, where a safe oral chelation agent is administered, and lead can be measured in the urine. Isotopic examination of the lead will often identify the source.
Queensland Health used to publish the number of non-occupational blood lead levels that exceeded 10 ug/dl (now 5 ug/dl)? I’ve looked and haven’t been able to find any numbers after 2015. There is a document, DOH-DL 17/18-048 that has recorded details about the issues of child lead levels up to 2018, but there have been no official notifications.
I know that Covid put huge pressures on Queensland Health to deal with a far more immediate health issue, but there are still children growing up in Mt Isa and it’s lead-affected satellite, Townsville, that are being harmed by the presence of raised levels of lead, some environmental, some due to lead paint on older houses. Maybe it’s time to revive the interest in reducing lead exposure as much as possible and possibly even treating sub-clinical cases of children with raised blood lead levels.
Broken Hill has a program where up to 80% of the children have their blood lead levels tested every year. This has been invaluable in the program to reduce lead exposure as much as possible. While similar programs exist in Mt Isa, less than 30% of Mt Isa children are tested and the urgency seems to have disappeared with the possible exception of opportunistic testing of left-over blood sample from children being tested for lead. Dr Steven Donohue convinced Queensland Health to do that, otherwise no one would have an idea of the extent of the problem. Existing voluntary testing levels are near non-exitent.
Mind you QH haven’t released the results, so we seem to have had at least 5 years of silence about the scale of lead poisoning in children in Mt. Isa.
QH need to wake up and realise that ignoring a silent epidemic of disease states due to lead affects everyone. It’s time to take notice rather than appear like they’ve closed ranks to avoid any suggestion that their lack of action might be doing harm.
There is a quote that may be relevant to the lead poisoning in children in Queensland and the relative inaction of Queensland Health:
“There can be no keener revelation of a society’s soul than the way in which it treats its children.” —Nelson Mandela
What kind of people are we if we are prepared to sacrifice children’s futures and health for a perceived economic gain? That’s what they do in third-world countries and sometimes not even there.
Why should we care about what’s happening in the US? Maybe because we might have a similar problem here, in places like Mt Isa and Townsville, where an unknown number of indigenous people have been affected by lead. We need to learn about what is happening in the US and think about the youth crime levels in our own lead cities.
The first quote is about Baltimore:
For more than a decade, Baltimore, which is 63 percent black, consistently has reported thousands of black children testing positive for lead poisoning, more than any other city in the state. Between 1993 and 2013, more than 65,000 children in Baltimore tested positive for dangerously high blood-lead levels.
Lack of funding from the federal government to address the threat of lead continues to have a detrimental impact on the safety of black residents. In 2015, the federal government slashed $35 million from the Office of Lead Hazard Control and Healthy Homes budget, which provides funding to state and local governments to help reduce the risk of lead poisoning. The cuts had a crippling effect in Baltimore’s ability to help its residents. As a result, Maryland’s Department of Environment and the federal Environmental Protection Agency found homes previously certified as “free of lead” were still contaminated or not tested at all. During that time, with less federal funding for lead prevention, Baltimore was left with just enough money to renovate only 230 homes out of thousands left as death traps.
Parts of America have a severe problem with older homes painted with lead paint, and the worst “lead” areas are near major highways where the areas were also severely contaminated with lead from leaded petrol. A large number of programs were set up with the intention of removing lead risk to children, things like a window exchange program because wooden windows with white lead paint were particularly attractive to young children, who licked the paint because it tasted sweet. There were also programs to remove interior lead paint, and other initiatives to remove lead hazards from children. Replacing lead pipes was also being done. Until 2015 when federal funding was slashed.
Despite the extensive evidence of the links between lead exposure and youth and later adult violence, and the overwhelming evidence of harmful neurological effects on children, the actions to reduce the outcomes of lead exposure essentially stopped.
In case you think it couldn’t happen here, ANY building constructed in Australia before 1970 is likely to have been painted with lead paint. There are suburbs near major highways in Sydney and Melbourne, that are so contaminated with lead it is unsafe to grow your own vegetables there.
Sydney University had glasshouses on top of buildings near a major highway. Following a hailstorm that damaged the glass, all the plants died, from lead poisoning. That’s actually quite a lot of lead which was deposited on top of the glass roofs of the glasshouse, until they were broken by hailstones
Were people affected? Probably, but as I’ve pointed out about the Borgias using lead to get rid of political rivals, lead is a slow and subtle poison.
A GP with a practice near a major highway in Sydney started getting blood lead tests done on his younger patients because he had become concerned with what lead might be doing. He was contacted by Medicare, who apparently threatened to rescind his provider number unless he stopped his frequent testing for lead.
There is NO wide-spread measurement of blood lead levels in children in Australia, with the possible exception of the lead cities.
Were you aware of the now closed Cockle Bay Smelter located at the northern end of Lake Macquarie near Boolaroo in Newcastle? Despite likely contamination of the surrounding area with lead, there is a new Costco centre on the site with are new housing developments proposed for the area.
If you want more stories, you’ll find them at (https://lead.org.au/). The the web site for the The Lead Education and Abatement Design Group, who have been trying for years to raise government awareness of the hazards of lead. I guess they are proof to me that a reasonable statement of facts about the dangers of lead might fail. But luckily I’m too stupid to give up.
I pointed out that there were many programs introduced to reduce the risk of lead in the United States, and to a lesser extent in the UK. Disregarding the fact that much of that funding has ceased, would it surprise you to learn that we’ve never had similar programs in Australia, with the possible exception of some lead reduction activities in Broken Hill and Mt Isa.
So let’s skip back to The Hill article:
According to the National Bureau of Economics, high levels of lead can cause increased school suspensions, juvenile incarcerations and criminal behavior as adults, and the National Center for Biotechnology Information (NCBI) found a link between lead and criminal and antisocial behavior. The research concluded: “With the exception of rape, aggregate blood-lead levels were statistically significant predictors of violent crime.”
The Mayo Clinic reports that lead poisoning in children causes numerous symptoms, including developmental delay, learning difficulties and irritability. Lead testing in Chicago, another city plagued by violence in black neighborhoods, revealed during a three-year period that 75 percent of Chicago’s elementary school students had high levels of lead.
To a large extent, the government has ignored the correlation between violent crime and lead poisoning. This negligence likely has contributed to the poor academic performance of black students, high rates of crime and ramped drug use. Federal, state and local governments must take a stronger, more definitive approach to eliminating the risks associated with high levels of lead in children living in inner-city neighborhoods.
If we consider that a significant number of children in Mt Isa have raised blood lead levels AND the highest levels are seen predominantly in aboriginal and islander children, when we think about the youth crime problems there, can you see any parallels?
I’ll finish up quoting the last parts of the article:
To a large extent, the government has ignored the correlation between violent crime and lead poisoning. This negligence likely has contributed to the poor academic performance of black students, high rates of crime and ramped drug use. Federal, state and local governments must take a stronger, more definitive approach to eliminating the risks associated with high levels of lead in children living in inner-city neighborhoods.
If politicians are genuinely outraged by the saturation of criminal activity in black communities, they cannot simply “mentor” or incarcerate their way to building safer communities. Instead, it is without question a necessity to address the environmental threats that feed the stereotype of black people living in struggling communities as poor, violent and uneducated. Lead poisoning is just as much a crisis as the nation’s opioid crisis that is now getting response from the Oval Office.
Pointing out the “usual suspects” and triggers of violence in poor black neighborhoods is ill-served when we ignore environmental hazards that can have a negative impact on generations of families.
Let’s state that again. Lead poisoning is as important, probably more so than the opioid crisis in the US. But it gets a lot less attention because the effects of lead are much more subtle.
And yet our government, with the possible exception of our work safety agencies who are grappling with a problem they don’t understand, and perhaps parts of NSW Health, ignore the community health issues relating to lead exposure.
Does the term criminal negligence come to mind?
Why is it so hard to admit you’re wrong, and to learn from other people’s mistakes if you are in government?
I’m sorry, but the diagram below seemed like the “perfect” way to leave a message about lead poisoning for Christmas. I used the term poisoning because the American CDC says no level of lead is “safe”. After all the Borgias used arsenic and lead for poisoning, with lead being the slower and more subtle way to kill your political enemies.
When you’re looking at the diagram below, you need to be aware that the symptoms or “results” of lead poisoning are dosage dependent. As the amount of lead in your body increases, more and more of this stuff happens.
Kind of like an advent calendar really. For each increment in blood lead levels, up pops a new disease. Not like Russian roulette because there you get 5 chances in 6 of something bad not happening. With lead bad things are guaranteed.
Another way to look at this is as follows:
Note all the stuff that happens when the BLL is below 10ug/dl. None of the effects on the nervous system are beneficial, most of them happen when your blood lead levels are UNDER 10 ug/dl.
Did I mention that gout is more common as blood lead levels increase?
At one time it was thought gout was a rich man’s disease, you got it because of overindulgence. But considering what drinking wine out of a pewter or lead crystal goblet might do to your blood lead levels, and only more well off people could afford pewter or lead crystal, is it a wonder rich people got gout more often?
It doesn’t say a lot more than I’ve said already but if you want an authoritative article about the harm from lead exposure, then this is almost rates. Let’s look at some of the figures:
The first is on the relationship between Blood lead level and loss of IQ in children. Losing 10 IQ points doesn’t seem like a big deal until you realise that it could be the difference between an adult coping with life and one that can’t.
The last time a group of children in Mt Isa had their blood lead levels tested almost 6 years ago, a fair percentage had BLL over 10ug/dl, some higher, though those were predominantly aboriginal and islander children. I had a cartoon in one of my earlier blogs that summarised this quite nicely.
If the BLL isn’t too high, affected kids will just be a bit slower, not quite as quick in picking things up. They’ll find school difficult and the school might very well find them difficult. They’ll be no smarter when they grow up, just even more difficult. Some of them will end up in jail because of the effects of lead. Not bad parenting, not bad genes, not a failure in the education system or the local community, but lead exposure.
I’d like to quote a short part of an article written by pediatricians about lead poisoning in Flint, Michigan and the effect of a drop in IQ caused by lead:
The effects of lead poisoning are not usually detected in a short visit with a doctor. The population impacts are, however, staggering. The consequences are one or two more kids in each classroom with symptoms of attention deficit hyperactivity disorder, 10 or 15 more kids in each school in special education programs, and fewer kids who are truly gifted. A five-point reduction in average IQ caused by widespread exposure to lead will result in a 50% increase in the number of children with IQ scores below 70 and a 50% decrease in the number with IQs higher than 130. In adults, lead exposure results in cardiovascular and kidney problems. And some studies have shown that children exposed to lead are at increased risk for school failure, unemployment, and incarceration.
We have children handicapped by lead exposure and despite knowledge that these children could potentially be helped, our health services do nothing. By nothing I don’t mean not necessarily removing lead but not doing any sort of rehabilitation. The human brain is wonderfully flexible and adaptable and with help a lot of degenerative defects can be worked around. But not even that is happening.
Actually, that statement isn’t quite accurate because there are a few clinics where an awareness of the effects of lead exists, and the benefits of lead removal are practiced. But good luck finding one.
My kids are grown up, and I haven’t been blessed with grandchildren, but if I did have grandchildren and they were living in Mt Isa, I suspect I’d be doing more than just writing a blog.
Let’s look at the graph of BLL vs cardiovascular mortality in adults. Nothing new here, but maybe a picture is better. This isn’t about cardiovascular disease which won’t necessarily kill you, this is about the risk of DYING of cardiovascular disease as your blood lead increases.
The scale on the left isn’t percentage it’s something called relative risk. At a BLL of 10 ug/dl, you have a 1.75 times greater risk of dying of cardiovascular disease, at 20ug/dl you have a 2 times better chance od dying of cardiovascular disease, and extrapolating to 30 ug/dl, that goes up to about 3 times. Are you really okay with having a BLL between 10-20 ug/dl? Are you silly enough to think that’s safe?
Think about hardening of the arteries, or maybe getting a foot amputated because of peripheral vascular disease and diabetes. If that’s not too thrilling, think about whether something could be done, which it can.
The picture below is of the foot of an 81-year old man with peripheral vascular disease and diabetes. His foot is just at the stage where amputation is going to be the next option.
On the top you’ve got quite obvious gangrenous toes where the foot was so painful the man couldn’t walk anymore. On the bottom you’ve got a healthy foot that is still attached, and able to be walked on. I think that’s pretty cool.
I pointed out that a Monash University study found a 7 times greater risk of oesophageal cancer at 30ug/dl BLL. That can result in also having your tongue cut out. Why would anyone be willing to risk that if they didn’t have to.
The Lancet article goes on to provide data for calculating the economic cost of lead exposure. There’s a lot of mathematical analyses, but the bottom line is that the economic cost of lead exposure is pretty massive. That makes the cost benefit analysis of removing lead versus doing nothing pretty conclusive.
And still we do nothing.
I’ll include a few direct quotes from the article:
The estimate of the global health burden of lead exposure in this study places lead exposure as an environmental risk factor at par with PM2·5 ambient and household air pollution combined, and ahead of unsafe household drinking water, sanitation, and handwashing
This states lead exposure beats air pollution when it comes to health costs. Doing something about exposure to lead is more imporatnt than safe drinking water or sanitation? You’ve got to be kidding, right?
Then again we don’t do anything about air pollution in Australia for the most part. Doesn’t it make you proud to realise we don’t give a damn about a lot of things that impact our health? Is that stoic or stupid?
The quote about LMICs below includes Austrlia. An LMIC is a low-to-middle-income-country.
A central implication for future research and policy is that LMICs bear an extraordinarily large share of the health and cost burden of lead exposure; consequently, improved quality of blood lead level measurements, lead exposure identification, research, policies, and practices are very urgently needed to address that burden.
Come on, we know what’s needed, health services that have an awareness of the dangers of lead, an awareness that lead is a causative factor in a lot of degenerative diseases and an awareness that sub-clinical lead poisoning needs to be treated.
If Queensland Health was on the ball, they’d have something to say about the flawed WHS policies. Actually F__KED WHS policies is a more apt description but we need to be a bit genteel here in case our authorities are too sensitive.
Well, I’ll try to end the year again.
Merry Christmas and a Happy New Year. Let’s hope something magic happens and we see a solution to this crazy WHS situation that keeps making things worse for people exposed to lead.
Knowledge about lead as a public health issue has increased substantially in the past few decades, but decision-making to deal with public health issues due to lead exposure has largely been absent.
The degree of public health protection enacted by our decision-makers can only be described as negligent. It is also apparent there is a huge difference between the acts of passing laws to minimise lead exposure and enforcing them.
As a result, lead affected children may be misdiagnosed with autism, lead exposure resulting in behavioural problems results in teenagers being jailed, and lead-affected adults suffer from a dizzying array of degenerative diseases before finishing up with lead-induced dementia if they don’t die of lead co-morbidities beforehand.
Think about the fact that lead paint has been banned, but is still in use in the automotive industry. Think of the fact that there is an EPA warning of the dangers of renovating pre-1980s homes, but no legislation to mandate appropriate care, like asbestos?
I learned a new acronym which is relevant to this continuing discussion, CSR. That’s not Colonial Sugar Refining but Corporate Social and Environmental Responsibility, which is an interesting concept.
In an ideal world CSR is intended to align a company’s social and environmental activities with it’s business purpose and values. In doing so CSR activities should mitigate risks, enhance reputation and contribute to business results.
Unless you’re a big mining company like Glencore of course.
I realise it’s pretty hard to generate a positive spin when it comes to environmental activities. I probably don’t need to give any examples to make this point, though I do have some since I’ve worked with a few mining companies in the past.
Still, an indication of a bit of social and moral responsibility would be nice. Being caught paying corrupt government officials with bags of cash kind of dampens the moral status of a company though, even if that’s the accepted way that business has to be done to get favorable prices for your commodities. I realise that you do business however you must, but openly carrying out corrupt behaviour does tarnish things a bit, even if everybody else does it too.
How about social responsibility then? I think I could argue that’s a failure as well. If you compare Glencore’s predecessors’ actions to Glencore’s, there is a marked difference. If someone comes to a company and presents irrefutable evidence that existing safety measures are harming employees of the company, is hiding behind misguided regulations the most responsible action? A sponsored pilot to gather information and develop alternatives would have been so much more responsible and enhanced their reputation. You don’t have to spend a lot of time on Glencore’s web site to be impressed with all their responsible actions. If you read some of the environmental comments about Mt Isa you won’t be impressed, though the miss the fat that the worst lead hazards in Mt isa are old houses.
They either don’t care, or equally likely are not allowed to care depending on the larger corporate culture. So we’re either dealing with people who don’t give a damn about worker health, or who are afraid to speak up because it will destroy their careers. That doesn’t say a lot of good things about their employer or work environment from a CSR viewpoint.
If the treatment of whistle-blowers (think ATO and ADF) is any indication, it takes a pretty special kind of person to lay it all on the line to reveal the unpalatable truth. The reaction of governments, who on the one hand praise whistle-blower’s activities and then jail them, makes it fairly clear that speaking up is a really bad idea. I’m pretty sure the same would go for company employees that cause embarrassment, even if black-listing someone in the industry isn’t quite as bad as jail, or is it? In this sort of environment, blaming employees for inaction seems somewhat unrealistic, even if doing nothing could result in significant harm to workers.
Even Universities and public broadcasters aren’t immune.
I can think of an instance where researchers from Newcastle University were testing water quality in Tasmanian rivers and were starting to find fairly extreme heavy metal contamination. One of the researchers talked about the results to a local (Hobart) radio station and the researchers were summarily recalled to Newcastle, the project terminated. Would it surprise you to learn that the only diagnosed case of Minamata disease (methylmercury poisoning) in Australia was in Tasmania?
The ABC had a science program called Catalyst that was pretty successful until the day they screened a couple of very-well researched and somewhat controversial programs about the usefulness and risks of statins. Pressure from outraged drug companies resulted in the crew that produced the programs being fired, and the Catalyst series being shut down.
So here we are, with things FUBAR to use a military term. We have a company where the acronym CSR (as defined above) has no meaning, government departments who are either too incompetent, spineless or corrupt to admit there might be a problem, and health services run by the 3 wise monkeys as far as lead is concerned.
What are the chances of a positive outcome in trying to inject a bit of sanity with regard to lead biohazard management and treatment for sub-clinical lead poisoning?
If I’m silly enough to be honest, pretty slim, but we’ll have to see. It turns out there are other people who care, and if enough of us can get together, who knows?
I think I’ll go fairly quiet over Christmas, but expect to hear more from me in the new year. People have remarked I’m too stupid to give up so who am I to argue.